A client's GTPAL is reviewed during her first prenatal visit. What does GTPAL represent?
Fetal measurements
Lab values
Pregnancy history
Weight gain
The Correct Answer is C
The GTPAL acronym is a standardized clinical tool used to document a woman’s obstetric history with precision. It tracks the total number of pregnancies and the specific outcomes of each, including gestational age at delivery. This data is vital for assessing obstetric risk in current and future pregnancies.
A. Fetal measurements: Anthropometric data such as crown-rump length or biparietal diameter are recorded during ultrasonography, not via the GTPAL system. These metrics assess fetal growth and developmental milestones. GTPAL focuses on the mother's historical reproductive events rather than current fetal size.
B. Lab values: Biochemical assessments like hemoglobin levels or blood type are separate components of the prenatal record. While important for clinical management, they are not captured by the GTPAL mnemonic. This tool is strictly for recording pregnancy occurrences and their timing.
C. Pregnancy history: GTPAL stands for Gravidity, Term births, Preterm births, Abortions, and Living children. This comprehensive summary allows providers to see at a glance the patient's reproductive performance and previous complications. It is the standard method for recording a longitudinal obstetric history.
D. Weight gain: Maternal weight changes are monitored using a gestational-tracking chart to ensure adequate nutrition and fetal development. These figures are recorded in kilograms or pounds during each visit. GTPAL does not include any data regarding maternal morphology or nutritional status.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The second stage of labor commences once the cervix achieves full dilation and complete effacement. This physiological milestone allows the fetal head to descend into the vaginal canal without causing cervical trauma or edema. Pushing prior to this stage can lead to cervical lacerations and maternal exhaustion.
A. At 10 cm dilation: Reaching 10 cm marks the transition from the first to the second stage of labor. At this point, the cervix is no longer palpable, providing a clear path for fetal descent. This ensures that maternal expulsive efforts are directed effectively toward delivery rather than pushing against an undilated cervical rim.
B. When contractions stop: The cessation of contractions indicates uterine atony or the end of the third stage of labor, not the time to begin pushing. Effective pushing requires the mechanical force of uterine contractions to move the fetus through the birth canal. Without these involuntary cycles, expulsive efforts are largely ineffective.
C. At 8 cm dilation: Attempting to push at 8 cm, which is still part of the transition phase, can cause the cervix to become edematous and swollen. This swelling may stall progress and necessitate a cesarean section due to cephalopelvic disproportion created by the inflamed tissue. It increases risk of uterine rupture.
D. Immediately on admission: Admission often occurs during the latent or active phases of the first stage of labor when dilation is minimal. Pushing at this early stage is premature and causes maternal fatigue long before the second stage is reached. It serves no clinical purpose and can cause fetal distress.
Correct Answer is A
Explanation
Umbilical cord prolapse occurs when the cord descends through the cervix ahead of the fetal presenting part. This mechanical compression leads to immediate fetal hypoxia due to the interruption of umbilical vein and artery blood flow. It constitutes an obstetric emergency requiring rapid decompression and surgical delivery.
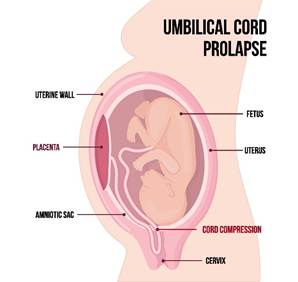
A. Elevate the presenting part: Manual upward pressure on the fetal head or breech relieves the mechanical compression on the prolapsed cord. This action preserves fetal oxygenation by maintaining patent umbilical vessels while preparing for an emergency cesarean section. It is the most critical immediate intervention to prevent fetal death.
B. Delay intervention: Any hesitation in a prolapse scenario leads to prolonged asphyxiation and irreversible neurological damage or intrauterine demise. The time between diagnosis and delivery must be minimized to ensure neonatal survival. Delaying treatment is a failure of standard clinical practice in emergency obstetrics.
C. Encourage pushing: Increasing maternal bearing-down efforts forces the fetus further into the pelvis, worsening the vascular occlusion of the cord. Pushing accelerates fetal distress and reduces the chances of a successful rescue. Efforts should focus on relieving pressure rather than advancing the second stage of labor.
D. Reposition to supine: The supine position allows gravity to further compress the cord against the pelvic brim and may cause aortocaval compression. Patients should instead be placed in a Trendelenburg or knee-chest position to help move the fetus away from the cervix. Supine positioning is detrimental in this clinical context.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today