A nurse is developing a plan of care for a client who has radiation-induced diarrhea and nausea. Which of the following interventions should the nurse include in the plan?
Provide a snack 30 min before treatments
Ensure foods are served hot
Administer antiemetics on a schedule
Serve low carbohydrate meals
The Correct Answer is C
Choice A reason: Providing a snack 30 min before treatments can worsen nausea and diarrhea, as food can stimulate gastric motility and secretion. It is better to avoid eating for at least 2 hours before and after treatments.
Choice B reason: Ensuring foods are served hot can increase nausea and diarrhea, as hot foods can have strong smells and irritate the digestive tract. It is better to serve foods at room temperature or cold.
Choice C reason: Administering antiemetics on a schedule can prevent nausea and vomiting, which can lead to dehydration and electrolyte imbalance. Antiemetics can also reduce abdominal cramps and spasms that cause diarrhea.
Choice D reason: Serving low carbohydrate meals can aggravate diarrhea, as carbohydrates are the main source of energy for the body. It is better to serve high carbohydrate meals that are easy to digest, such as rice, potatoes, bread, or crackers.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
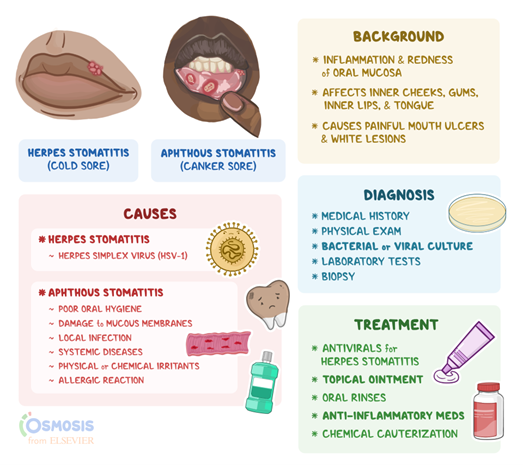
Choice A reason: Offering the client frozen banana as a snack is an appropriate intervention for the nurse to take because it can help soothe and cool the inflamed mucous membranes in the mouth and throat, which are caused by stomatitis. Stomatitis is an inflammation of the oral cavity that can result from radiation therapy or chemotherapy. Frozen banana also provides potassium, vitamin C, and fiber for the client.
Choice B reason: Serving the client hot meals is not an appropriate intervention for the nurse to take because it can worsen nausea and vomiting. Hot meals are aromatic, spicy, and greasy, which are characteristics of emetic foods. Hot meals can also irritate the stomach lining and trigger the gag reflex.
Choice C reason: Avoiding serving sauces or gravies is not an appropriate intervention for the nurse to take because it can cause dehydration and malnutrition. Sauces and gravies are liquid, mild, and moist, which are characteristics of antiemetic foods. Sauces and gravies can also enhance the flavor and texture of bland foods and provide calories and nutrients for the client.
Choice D reason: Discouraging the use of a straw is not an appropriate intervention for the nurse to take because it can prevent adequate fluid intake and hydration. Using a straw can help the client sip small amounts of clear liquids, such as water, ginger ale, or broth, which are antiemetic fluids. Using a straw can also reduce the exposure to odors and tastes that may cause nausea.
Correct Answer is D
Explanation
Choice A reason: The client's creatinine level of 1.0 mg/dL is within the normal range (0.6-1.2), but it does not indicate the effectiveness of the treatment for benign prostatic hyperplasia. Creatinine is a waste product of muscle metabolism that is filtered by the kidneys. High creatinine levels can indicate kidney damage or impaired renal function.
Choice B reason: The client's urine output of 35 mL/hr is below the normal range (40-60), and it indicates the need for further assessment. Low urine output can indicate dehydration, urinary retention, or kidney failure.
Choice C reason: The client's stool consistency and color are not related to the treatment for benign prostatic hyperplasia. Soft, brown stool is normal and does not indicate any problem with the digestive system.
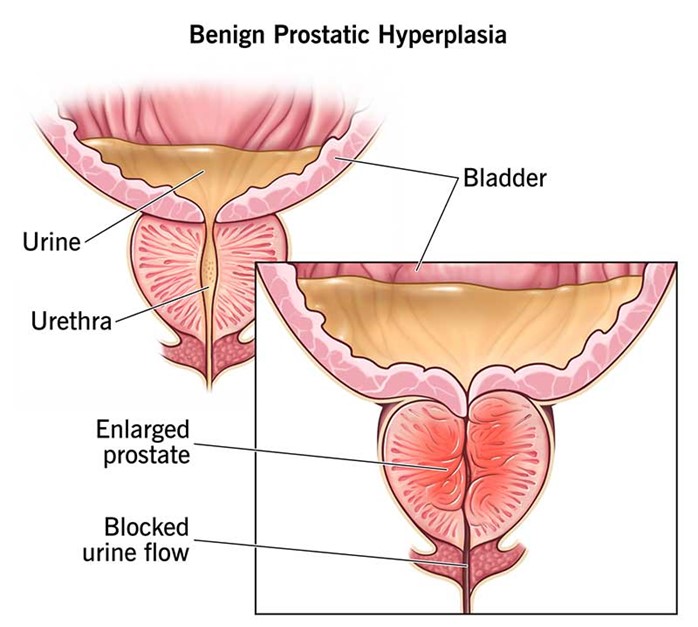
Choice D reason: The client's ability to urinate without straining indicates that the treatment for benign prostatic hyperplasia has been effective. Benign prostatic hyperplasia is a condition in which the prostate gland enlarges and compresses the urethra, causing difficulty in urination. Treatment options include medication, surgery, or minimally invasive procedures to reduce the size of the prostate and relieve urinary obstruction.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today