The psychiatric nurse is caring for clients on an adolescent unit. Which client requires the nurse's immediate attention?
A 16-year-old client diagnosed with major depression who refuses to participate in group.
A 17-year-old client diagnosed with bipolar disorder who is pacing around the lobby.
An 18-year-old client with antisocial behavior who is being yelled at by other clients.
A 14-year-old client with anorexia nervosa who is refusing to eat the evening snack.
None
None
The Correct Answer is B
Choice A reason: A 16-year-old client diagnosed with major depression who refuses to participate in group does not require the nurse's immediate attention. Depression is a mood disorder that causes persistent feelings of sadness, hopelessness, and loss of interest. Refusing to participate in group may indicate low motivation, social withdrawal, or poor self-esteem, which are common symptoms of depression. The nurse should respect the client's preference and offer alternative activities or individual therapy.
Choice B reason: This client requires immediate intervention because pacing can be a sign of agitation, restlessness, or escalating mania. Clients with bipolar disorder in a manic phase may exhibit increased energy, impulsivity, irritability, and even aggression. If not addressed promptly, this behavior could escalate to disruptive outbursts, impulsive actions, or even violence toward themselves or others. The nurse should intervene by using calm communication, redirection, and possibly medication if prescribed to help de-escalate the situation and ensure safety.
Choice C reason: This scenario involves peer conflict, which is important to address, but it does not necessarily indicate an immediate risk of harm. Clients with antisocial behavior often engage in conflict due to manipulative or confrontational tendencies, but being yelled at does not mean they are in immediate danger. The nurse should monitor the situation and intervene to prevent escalation, but other safety concerns take priority.
Choice D reason: A 14-year-old client with anorexia nervosa who is refusing to eat the evening snack does not require the nurse's immediate attention. Anorexia nervosa is an eating disorder that causes extreme restriction of food intake and fear of weight gain. Refusing to eat the evening snack may indicate distorted body image, dietary rules, or anxiety, which are common factors of anorexia nervosa. The nurse should encourage the client to eat and provide support and education.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Securing chest tube to the stretcher for transport is a good practice, but it is not the most important action. The chest tube should be secured to prevent accidental dislodgement or kinking, but it does not affect the function of the chest tube or the drainage system.
Choice B: Administering PRN pain medication prior to transport is a compassionate action, but it is not the most important action. The client may experience pain due to the chest tube, the intubation, or the underlying condition, but pain relief is not a priority over maintaining adequate ventilation and drainage.
Choice C: Marking the amount of chest drainage on the container is a useful action, but it is not the most important action. The amount of chest drainage should be recorded and reported to monitor the client's status and detect any complications, such as hemorrhage or infection, but it does not affect the immediate function of the chest tube or the drainage system.
Choice D: Keeping the chest tube container below the site of insertion is the most important action for the nurse to take. The chest tube container should be kept below the level of the client's chest to maintain a gravity-dependent pressure gradient that allows air and fluid to drain from the pleural space. If the container is raised above the site of insertion, it can cause backflow of air or fluid into the pleural space, which can compromise ventilation and cause tension pneumothorax.
Correct Answer is A
Explanation
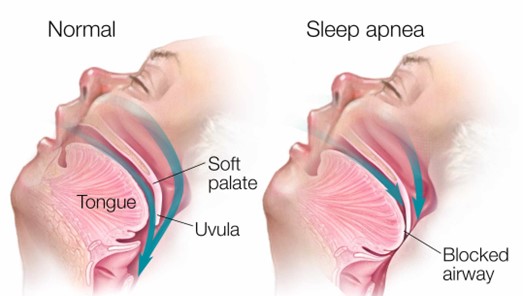
Choice B reason: Elevating the head of the bed to a 45-degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as a positive airway pressure device, weight loss, or surgery.
Choice C reason: Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
Choice D reason: Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today