Neurodegenerative Diseases: Alzheimer's disease, Parkinson's disease
- Neurodegenerative diseases are a group of chronic progressive disorders that result from the loss or dysfunction of neurons in specific regions of the brain
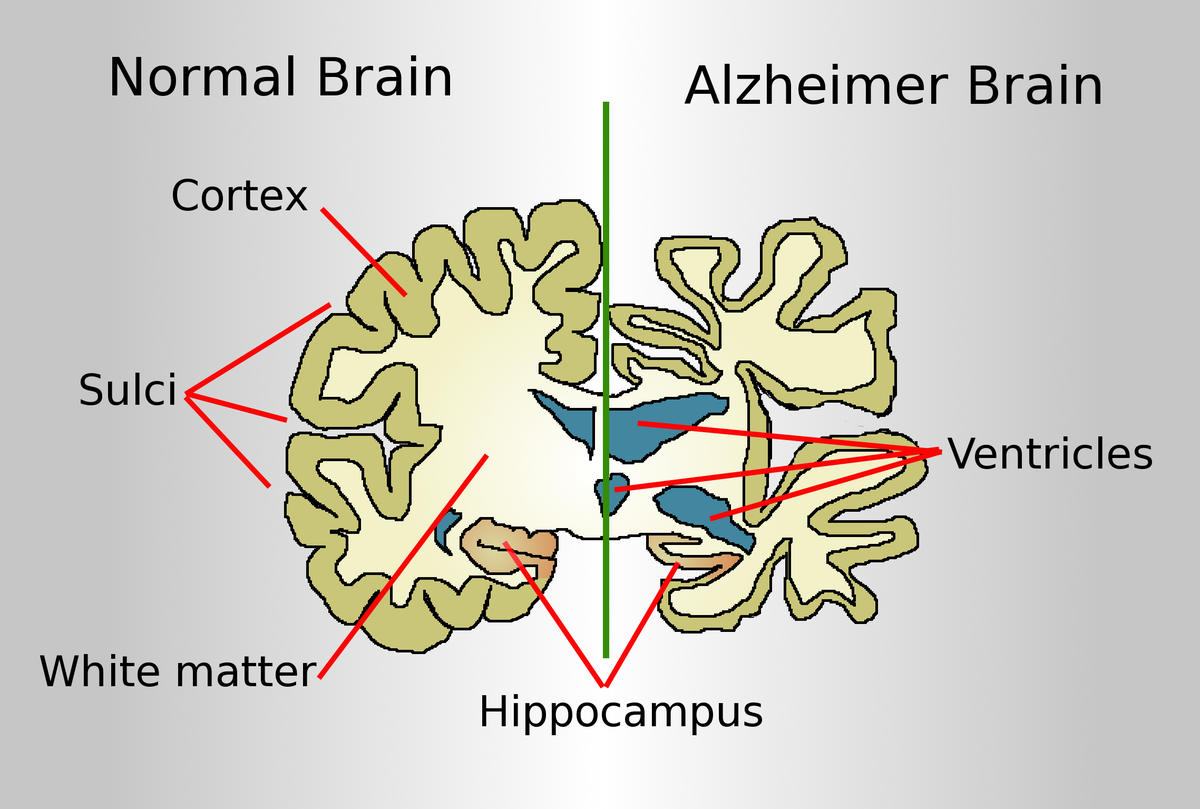
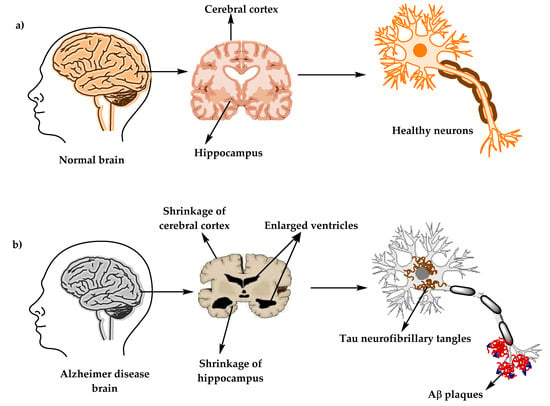
- Alzheimer’s disease (AD) is the most common cause of dementia in older adults. It is characterized by the accumulation of amyloid plaques and neurofibrillary tangles in the cerebral cortex, leading to cognitive impairment, memory loss, behavioral changes, and functional decline
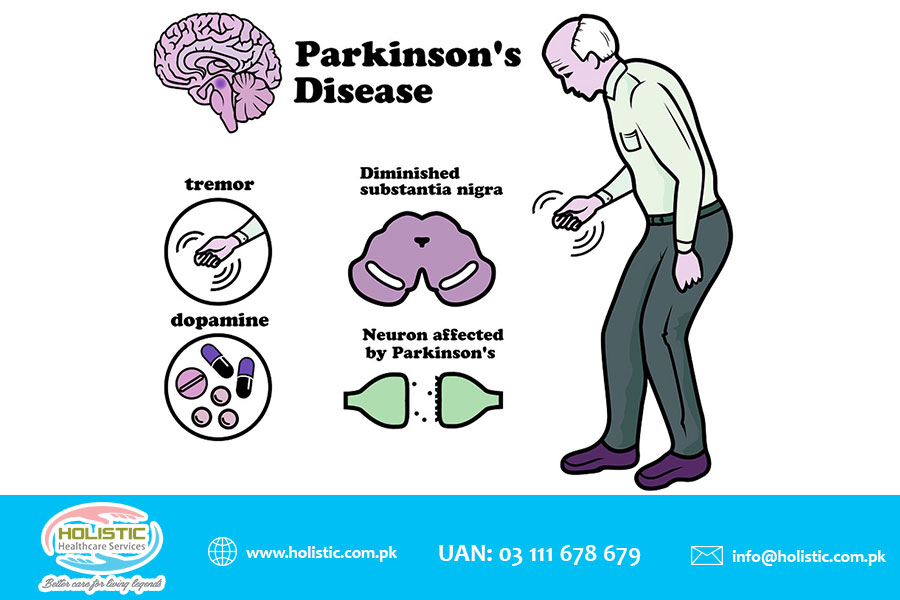
- Parkinson’s disease (PD) is a movement disorder that affects the basal ganglia. It is characterized by the degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNpc), leading to motor symptoms such as tremor, rigidity, bradykinesia (slowness of movement), postural instability (balance problems), and non-motor symptoms such as depression, anxiety, sleep disorders, autonomic dysfunction (e.g., constipation), etc.
- The exact causes of AD and PD are unknown. However, some possible risk factors include:
- Age: The risk of developing AD or PD increases with advancing age
- Genetics: Some forms of AD or PD are inherited or associated with specific gene mutations or variants
- Environmental factors: Exposure to toxins (e.g., pesticides), head trauma, infections (e.g., viral encephalitis), oxidative stress (e.g., free radicals), inflammation (e.g., chronic systemic diseases), etc. may contribute to neuronal damage or dysfunction
- Lifestyle factors: Smoking, alcohol consumption, poor diet, physical inactivity, cognitive inactivity, etc. may increase the risk or worsen the progression of AD or PD
- The signs and symptoms of AD or PD vary depending on the stage and severity of the disease. Some common manifestations include:
- Alzheimer’s disease (AD:
- Mild cognitive impairment (MCI): The earliest stage of AD that involves subtle changes in memory or thinking that do not interfere with daily activities
- Mild AD: The stage of AD that involves noticeable memory loss (especially short-term memory), difficulty with language (e.g., word-finding problems), visuospatial skills (e.g., getting lost), executive functions (e.g., planning), judgment, reasoning, etc. that affect daily functioning
- Moderate AD: The stage of AD that involves more severe cognitive impairment that affects long-term memory, orientation, recognition, calculation, etc. as well as behavioral changes such as agitation, irritability, mood swings, delusions, hallucinations, etc.
- Severe AD: The stage of AD that involves profound cognitive impairment that affects all aspects of mental functioning as well as functional decline that requires total dependence on others for basic activities of daily living (ADLs) such as eating, dressing, bathing, toileting, etc.
- Alzheimer’s disease (AD:
- Parkinson’s disease (PD):
- Advanced PD: The stage of PD that involves severe motor complications such as dyskinesia (involuntary movements), dystonia (abnormal muscle tone), freezing (sudden inability to move), wearing-off (reduced duration of medication effect), on-off (fluctuations between mobility and immobility), etc. as well as non-motor complications such as cognitive impairment, dementia, psychosis, etc.
- Clinical PD: The stage of PD that involves the presence of motor symptoms that are typically asymmetric and respond to dopaminergic therapy. The motor symptoms are classified into four cardinal features: tremor, rigidity, bradykinesia, and postural instability. The severity of the motor symptoms is assessed by the Hoehn and Yahr scale, which ranges from stage 1 (unilateral involvement) to stage 5 (wheelchair-bound or bedridden)
- Prodromal PD: The stage of PD that occurs when the motor symptoms are not yet clinically detectable but can be identified by specialized tests such as neuroimaging or biomarkers
- Preclinical PD: The stage of PD that occurs before the onset of motor symptoms and involves non-motor symptoms such as loss of smell (anosmia), constipation, depression, anxiety, REM sleep behavior disorder (RBD), etc.
- The diagnosis of AD or Parkinson’s disease (PD) is based on clinical criteria that include medical history, physical examination, neurological examination, cognitive assessment, and exclusion of other possible causes. Some diagnostic tests that may be used to support the diagnosis or rule out other conditions include:
- Alzheimer’s disease (AD:
- Blood tests: To check for vitamin B12 deficiency, thyroid dysfunction, infection, etc.
- Urinalysis: To check for urinary tract infection, dehydration, etc.
- Lumbar puncture: To measure the levels of amyloid beta and tau proteins in the cerebrospinal fluid (CSF) that may indicate AD
- Neuroimaging: To visualize the structure and function of the brain using techniques such as computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), single-photon emission computed tomography (SPECT), etc. that may show atrophy (shrinkage) or hypometabolism (reduced activity) of specific brain regions affected by AD
- Neuropsychological testing: To assess the cognitive domains such as memory, language, visuospatial skills, executive functions, etc. using standardized tools such as the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog), etc.
- Parkinson’s disease (PD):
- Blood tests: To check for infection, electrolyte imbalance, liver or kidney function, etc.
- Urinalysis: To check for infection, dehydration, etc.
- Lumbar puncture: To measure the levels of alpha-synuclein protein in the CSF that may indicate PD
- Neuroimaging: To visualize the structure and function of the brain using techniques such as CT, MRI, PET, SPECT, etc. that may show loss or dysfunction of dopaminergic neurons in the SNpc or other brain regions affected by PD
- Neuropsychological testing: To assess the cognitive domains such as attention, memory, language, visuospatial skills, executive functions, etc. using standardized tools such as the MMSE, MoCA, Parkinson’s Disease Cognitive Rating Scale (PD-CRS), etc.
- DaTscan: A specific type of SPECT scan that uses a radioactive tracer that binds to dopamine transporters in the brain and can detect reduced dopamine uptake in the striatum (a part of the basal ganglia) that is characteristic of PD
- Alzheimer’s disease (AD:
- The treatment of AD or PD is aimed at slowing down the progression of the disease, managing the symptoms, improving the quality of life, and providing support and education for the patient and caregivers. Some treatment options include:
- Alzheimer’s disease (AD:
- Pharmacological therapy: To enhance or modulate neurotransmitter activity in the brain using drugs such as cholinesterase inhibitors (e.g., donepezil, rivastigmine, galantamine) that increase acetylcholine levels or N-methyl-D-aspartate (NMDA) receptor antagonists (e.g., memantine) that block glutamate excitotoxicity. These drugs may improve cognition, behavior, and function in mild to moderate AD but have limited efficacy and side effects such as nausea, vomiting, diarrhea, headache, dizziness, etc.
- Non-pharmacological therapy: To stimulate or maintain cognitive abilities and social interactions using interventions such as cognitive stimulation therapy (CST), reminiscence therapy, music therapy, art therapy, etc. that involve engaging in meaningful activities, recalling past experiences, expressing emotions, etc. These interventions may enhance mood, self-esteem, communication, and well-being in AD patients and caregivers - Behavioral therapy: To manage or modify behavioral symptoms such as agitation, irritability, aggression, wandering, etc. using interventions such as validation therapy, reality orientation, redirection, distraction, environmental modification, etc. that involve acknowledging the patient’s feelings, providing orientation cues, diverting attention to other activities, creating a safe and comfortable environment, etc. These interventions may reduce stress, anxiety, and frustration in AD patients and caregivers - Physical therapy: To improve or maintain physical function and mobility using interventions such as exercise, stretching, balance training, gait training, etc. that involve performing physical activities that are appropriate for the patient’s condition and preferences. These interventions may prevent or delay complications such as falls, fractures, pressure ulcers, contractures, etc. and improve cardiovascular health, muscle strength, flexibility, and endurance in AD patients - Occupational therapy: To improve or maintain daily living skills and independence using interventions such as task analysis, task simplification, assistive devices, environmental adaptation, etc. that involve breaking down complex tasks into simpler steps, reducing the cognitive demands of tasks, providing aids or tools to facilitate tasks, modifying the environment to suit the patient’s needs and abilities, etc. These interventions may enhance self-care, productivity, leisure, and safety in AD patients - Speech therapy: To improve or maintain communication and swallowing skills using interventions such as language stimulation, cueing, prompting, alternative or augmentative communication (AAC) devices, swallowing exercises, diet modification, etc. that involve providing verbal or non-verbal cues to elicit responses, repeating or rephrasing words or sentences, using pictures or symbols to convey messages, performing oral motor exercises to strengthen the muscles involved in swallowing, changing the texture or consistency of food or liquids to facilitate swallowing, etc. These interventions may prevent or reduce communication difficulties, social isolation, aspiration pneumonia, malnutrition, dehydration, etc. in AD patients
- Alzheimer’s disease (AD:
- Parkinson’s disease (PD):
- Non-pharmacological therapy: To manage or reduce non-motor symptoms and complications using interventions such as deep brain stimulation (DBS), transcranial magnetic stimulation (TMS), physical therapy, occupational therapy, speech therapy, cognitive behavioral therapy (CBT), mindfulness-based stress reduction (MBSR), etc. that involve stimulating specific brain regions with electrical currents or magnetic fields to modulate neuronal activity, improving physical function and mobility, enhancing daily living skills and independence, improving communication and swallowing skills, addressing psychological issues such as depression, anxiety, etc., reducing stress and improving coping skills, etc. These interventions may improve quality of life and well-being in PD patients and caregivers
- Pharmacological therapy: To restore or modulate dopamine activity in the brain using drugs such as levodopa (L-dopa), carbidopa, dopamine agonists (e.g., pramipexole, ropinirole), monoamine oxidase B (MAO-B) inhibitors (e.g., selegiline, rasagiline), catechol-O-methyltransferase (COMT) inhibitors (e.g., entacapone), anticholinergics (e.g., trihexyphenidyl), etc. These drugs may improve motor symptoms and function in PD patients but have side effects such as nausea, vomiting, orthostatic hypotension (low blood pressure when standing up), dyskinesia, psychosis, etc.
- The prevention of Alzheimer’s disease (AD) or Parkinson’s disease (PD) is not fully established. However, some possible preventive measures include:
- Maintaining a healthy lifestyle: Eating a balanced diet rich in antioxidants (e.g., fruits, vegetables), omega-3 fatty acids (e.g., fish), and vitamins (e.g., B12), avoiding smoking and excessive alcohol consumption, exercising regularly (at least 150 minutes per week of moderate-intensity aerobic activity), managing chronic conditions such as hypertension, diabetes, hyperlipidemia (high cholesterol), etc., getting enough sleep (7-9 hours per night), and avoiding head injuries
- Engaging in cognitive and social activities: Reading books, playing games, learning new skills, taking courses, volunteering for a cause, joining a club or group, maintaining social contacts with family and friends, etc.
- Seeking medical attention: Consulting a doctor if experiencing any signs or symptoms of AD or PD or having a family history of these diseases
Diagnosis of AD or Parkinson’s disease (PD)
Treatment of AD or Parkinson’s disease (PD)
Nursing Test Bank
Test Bank #1: RN Pharmacology Exams
Test Bank #2: RN Medical-Surgical Exams
Test Bank #3: RN Fundamentals Exams
Test Bank #4: RN Maternal-Newborn Exams
Test Bank #5: RN Anatomy and Physiology Exams
Test Bank #6: RN Obstetrics and Pediatrics Exams
Test Bank #7: RN Fluid and Electrolytes Exams
Test Bank #9: RN Adult Health
Test Bank #10: RN Dosage Calculation
Test Bank #11: RN Community Health Exams
Test Bank #12: RN Psychology Exams
Test Bank #13: RN Nursing Care Of Children
Test Bank #14: RN Foundations of Nursing Exams
Naxlex Comprehensive Predictor Exams
Exam #1: RN Comprehensive predictor 2023 proctored exam
Exam #2: Ati rn vati comprehensive predictor proctored exam
Exam #3: Ati Rn Comprehensive Predictor Proctored Exam 2023
Exam #4: Rn Comprehensive Predictor 2023 Proctored Exam - St. Joseph
Exam #5: RN Comprehensive Predictor Proctored Exam (National U CA San Diego)
Exam #6: Ati rn comprehensive predictor 2023 retake proctored exam
Exam #7: RN Hesi Exit Proctored Exam
Exam #8: Hesi RN Exit proctored exam
Exam #9: Hesi rn exit proctored exam
Exam #10: Hesi Rn compass exit B proctored exam
Questions on Neurodegenerative Diseases: Alzheimer's disease, Parkinson's disease
Correct Answer is C
Explanation
This is an incorrect answer. The caregiver does not need further teaching if they say that memantine will help slow down the decline of their loved one's cognitive function. Memantine can slow down the progression of AD and delay the need for institutionalization by preserving some cognitive abilities and daily functioning.
Correct Answer is D
Explanation
This is a correct answer. The caregiver needs further teaching if they say that pramipexole will help improve the mood and motivation of their loved one. This is not the purpose or effect of pramipexole, but rather antidepressants or stimulants, which are medications used to treat depression or apathy, respectively. Depression or apathy are common neuropsychiatric symptoms of PD, which affect the levels of serotonin, norepinephrine, or dopamine in the brain.
Correct Answer is ["A","B","C","D"]
Explanation
This is an incorrect answer. Nuchal rigidity is not a common symptom of PD, but rather a sign of meningitis or subarachnoid hemorrhage. Nuchal rigidity occurs when there is stiffness or pain in the neck when flexing or extending it due to inflammation or irritation of the meninges or subarachnoid space.
Correct Answer is B
Explanation
This is an incorrect answer. The nurse should not instruct the client to take levodopa-carbidopa as needed when they have symptoms of PD. This is not an appropriate way to take levodopa-carbidopa, as it can cause erratic changes in dopamine levels and worsen the symptoms and progression of PD. The nurse should advise the client to take levodopa-carbidopa as prescribed by their provider and not to skip or adjust doses without consulting their provider.