
Growth And Development In Toddlers
Lessons
Notes Highlighting is available once you sign in. Login Here.
Objectives
- Articulate the key developmental milestones across biologic, cognitive, moral, spiritual, body image, gender identity, and social domains in toddlers (ages 1-3 years).
- Identify nursing interventions that promote optimum growth and development in toddlers, considering their unique needs and vulnerabilities.
- Discuss common concerns related to normal toddler growth and development.
- Analyze the impact of temperament on toddler behavior and development, and apply this understanding to individualized nursing care.
- Develop evidence-based strategies for promoting optimum health during toddlerhood, encompassing nutrition, sleep, activity, dental health, and injury prevention.
- Integrate knowledge of complementary and alternative medicine (CAM) and vegetarian diets into the nutritional counseling of parents of toddlers, recognizing potential benefits and risks.
- Educate parents and caregivers on age-appropriate safety measures to prevent common injuries in toddlers.
- Apply the nursing process to assess, plan, implement, and evaluate care for toddlers and their families, fostering healthy growth and development.
Introduction
- Toddlerhood, spanning the ages of 12 months to 36 months, is a period of remarkable growth and rapid development.
- Characterized by increasing autonomy, burgeoning language skills, and significant physical advancements, toddlers transition from dependent infants to increasingly independent individuals.
- This stage is crucial for establishing foundational cognitive, social, and emotional skills that will influence future development.
- Nurses play a vital role in supporting families during this transformative period, providing anticipatory guidance, promoting healthy behaviors, and addressing common developmental challenges.
- Understanding the nuances of toddler growth and development is paramount for delivering comprehensive and effective nursing care.
Promoting Optimum Growth And Development
- Promoting optimum growth and development in toddlers requires a holistic approach, considering all aspects of their physical, cognitive, social, and emotional well-being.
- Nurses act as educators, advocates, and care providers, guiding parents through this dynamic stage.
1.1. Biologic Development
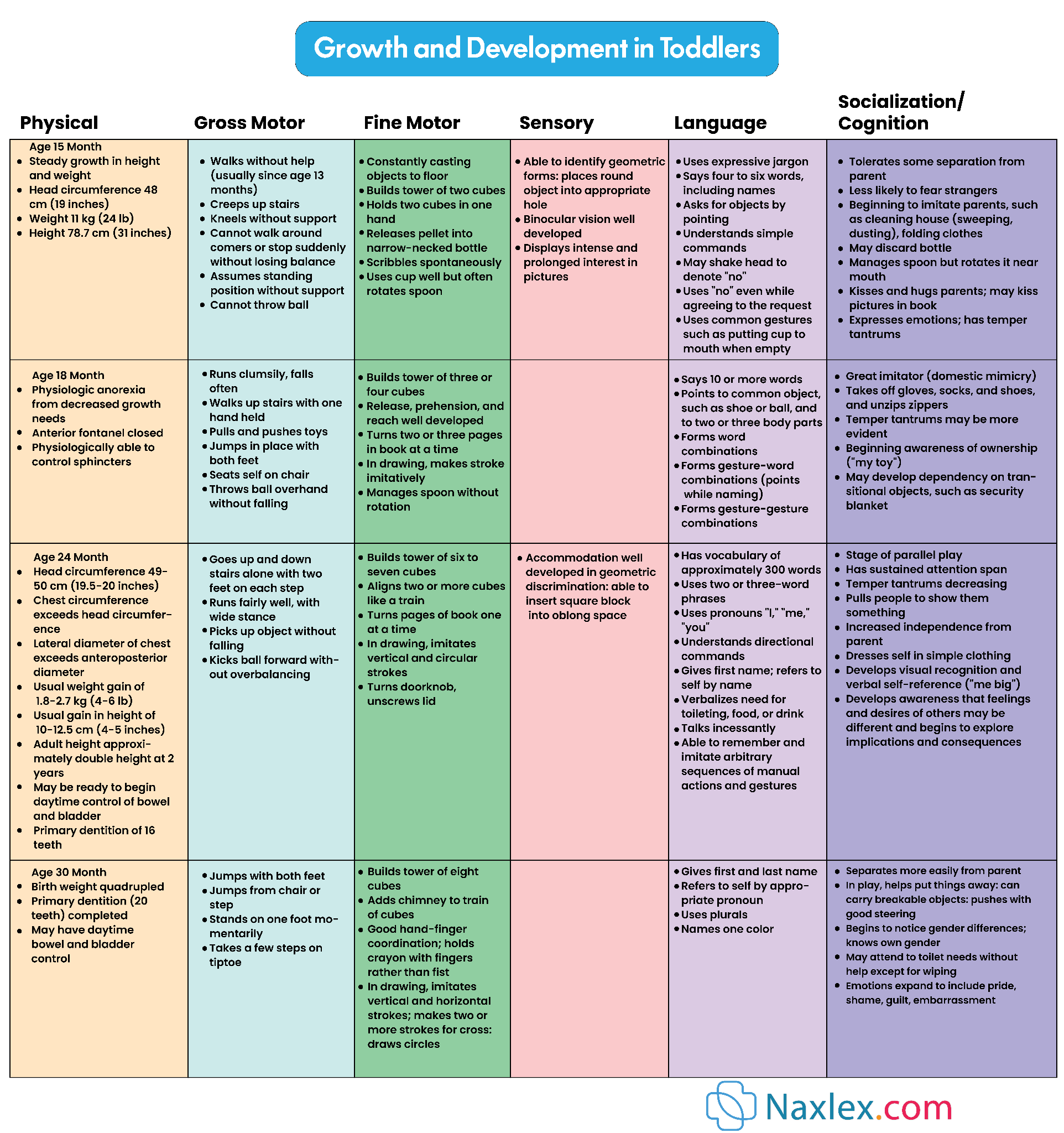
- Biologic development in toddlers is marked by significant physical growth and maturation of body systems. While growth slows compared to infancy, it remains rapid.
- Weight: On average, toddlers gain approximately 4 to 6 pounds (1.8 to 2.7 kg) per year. By 2.5 years, their birth weight has quadrupled.
- Height: Toddlers grow about 3 inches (7.5 cm) per year.
- Head Circumference: Head growth continues, but at a slower pace than in infancy, reflecting continued brain development. By 2 years, head circumference is typically 90% of adult size.
- Fontanels: The anterior fontanel typically closes between 12 and 18 months of age.
- Body Proportions: The toddler's body proportions change, with the trunk and extremities growing faster, giving them a more elongated appearance than infants.
Nursing Insight: Deviations from expected growth curves such as weight, height, and head circumference can signal underlying health issues requiring further investigation.
- Gross Motor Skills:
- 12-15 months: Walks independently, creeps up stairs, stands without support, stoops and recovers.
Typical Toddler Gait

- 18 months: Runs stiffly, throws a ball overhand (without much accuracy), jumps in place with both feet, pulls/pushes toys.
- 24 months: Walks up and down stairs holding on, kicks a ball forward, stands on tiptoes, builds a tower of 6-7 blocks.
- 30 months: Jumps with both feet, stands on one foot momentarily, takes a few steps on tiptoes.
- 36 months: Rides a tricycle, alternates feet going up stairs, jumps over objects.
- Fine Motor Skills:
- 12-15 months: Uses a cup well, builds a tower of 2 blocks, scribbles spontaneously.
- 18 months: Manages a spoon without rotating, turns pages in a book (two or three at a time), builds a tower of 3-4 blocks, imitates drawing a vertical line.
- 24 months: Builds a tower of 6-7 blocks, imitates drawing a horizontal line, completes simple puzzles (3-4 pieces), unbuttons large buttons.
- 30 months: Draws circles, copies a cross, builds a tower of 8 blocks.
- 36 months: Copies a circle, draws a person with 2-3 parts, uses blunt scissors.
- Physiological Systems:
- Respirations: Slows to 25-30 breaths per minute. Airways are still relatively small, making toddlers susceptible to respiratory infections.
- Heart Rate: Slows to 80-110 beats per minute.
- Blood Pressure: Increases to approximately 90/50 mmHg.
- Thermoregulation: Improves but toddlers are still vulnerable to extreme temperatures.
- Immune System: Continues to mature, but toddlers still experience frequent infections, especially if in group childcare settings. Maternal antibodies are decreasing.
- Gastrointestinal System: Digestive processes mature, allowing for a wider variety of foods. Bowel control develops later.
- Renal System: Kidneys mature, and bladder capacity increases, contributing to readiness for toilet training.
Nursing Implications for Biologic Development:
- Monitor growth parameters (weight, height, head circumference) regularly and plot on growth charts.
- Provide anticipatory guidance on age-appropriate gross and fine motor skill development.
- Encourage opportunities for active play and exploration to enhance motor development.
- Educate parents on normal physiological changes and signs of illness.
- Advise on appropriate sleep patterns and rest.
- Emphasize the importance of a balanced diet for optimal physical growth.
1.2. Cognitive Development (Piaget: Sensorimotor and Preoperational Phases)
Toddlers are in the latter part of Piaget's sensorimotor stage and are transitioning into the preoperational stage.
- Sensorimotor Stage (12-24 months):
- Tertiary Circular Reactions (12-18 months): Toddlers actively experiment with objects, trying out new behaviors to see what happens (e.g., dropping a spoon repeatedly). They use trial-and-error to solve problems.
- Invention of New Means Through Mental Combinations (18-24 months): Toddlers begin to think before they act. They can solve problems in their minds and understand cause-and-effect relationships more abstractly. Object permanence is fully developed. They engage in domestic mimicry (imitating household activities).
- Preoperational Stage (2-7 years):
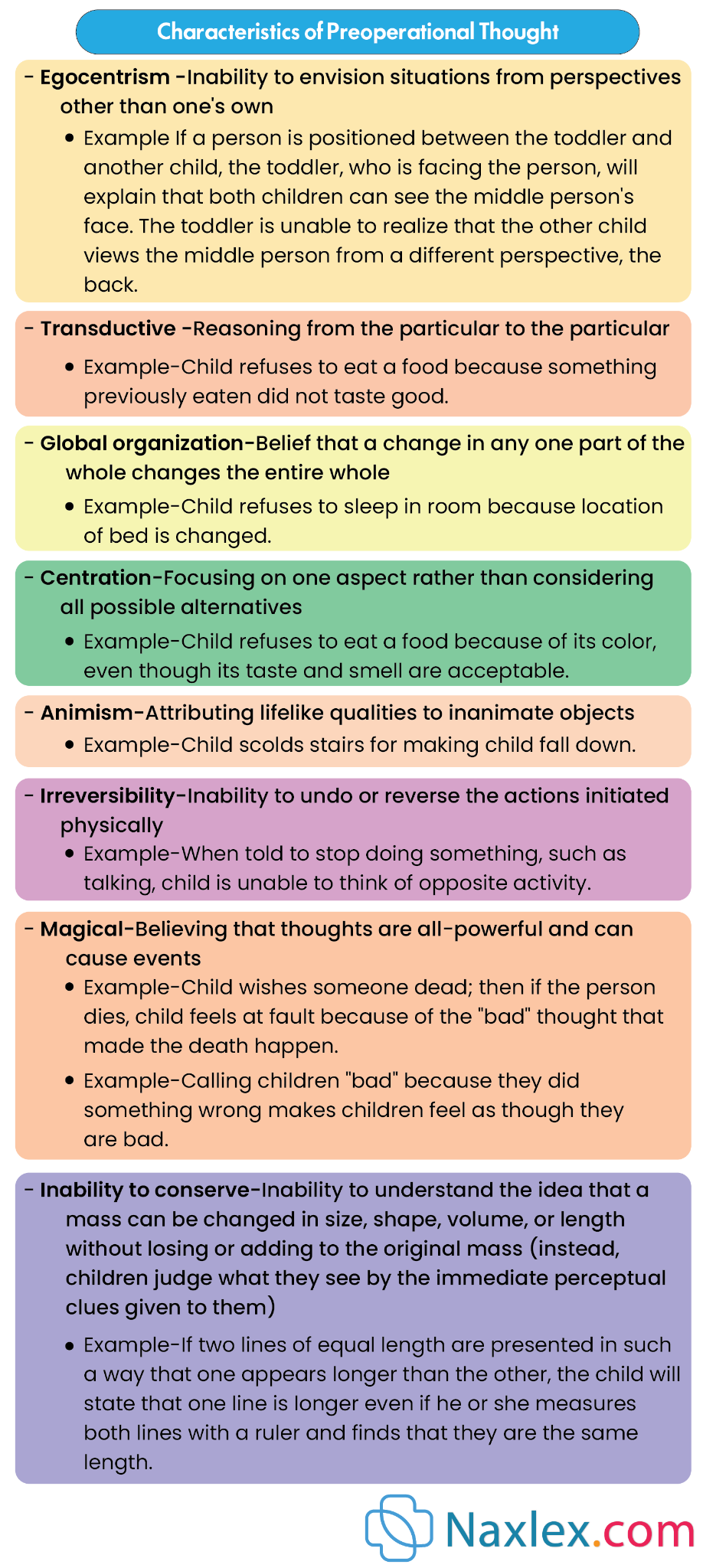
- Preconceptual Phase (2-4 years): This phase is marked by the beginning of symbolic thought.
- Egocentrism: Toddlers are unable to see situations from another person's perspective. They believe everyone sees the world as they do.
- Transductive Reasoning: Toddlers connect particular experiences, whether or not there is a logical casual relationship (e.g., "The sun sets because I go to bed").
- Animism: Attributing lifelike qualities to inanimate objects (e.g., "The doll is sad").
- Magical Thinking: Believing that thoughts or actions can cause events to happen (e.g., "If I wish for it, it will happen").
- Global Organization: If one aspect of a situation changes, the whole situation changes (e.g., new clothes mean a new identity).
- Centration: Focusing on one aspect of a situation and neglecting other important features.
- Irreversibility: Inability to mentally reverse a sequence of events or operations.
- Preconceptual Phase (2-4 years): This phase is marked by the beginning of symbolic thought.
Characteristics of Preoperational Thought
- Language Development:
- 12-15 months: Uses 4-6 words, imitates animal sounds, babbles with inflection.
- 18 months: Uses 10-20 words, uses two-word phrases ("want cookie"), points to familiar objects.
- 24 months: Uses 300 words, uses 2-3 word sentences, asks "what?" and "where?" questions, names familiar objects and body parts.
- 36 months: Uses 900-1000 words, uses 3-4 word sentences, uses pronouns (I, you, me), understands most of what is said, can give first name and age.
- Concept of Time and Space: Still limited to "now" and "here."
- Problem Solving: Moves from trial and error to more thoughtful approaches.
Nursing Implications for Cognitive Development:
- Provide opportunities for play that encourages exploration and problem-solving (e.g., stacking toys, simple puzzles).
- Engage in conversations with toddlers, encouraging language development through repetition, clear pronunciation, and expanding on their utterances.
- Read aloud to toddlers daily to foster language and cognitive skills.
- Acknowledge and respect their egocentric perspective, understanding it's a normal part of development.
- Use simple, concrete language when communicating with toddlers.
- Explain procedures in a way they can understand, using their level of cognitive development.
1.3. Moral Development - Preconventional or Premoral Level (Kohlberg)
According to Kohlberg, toddlers are in the preconventional or premoral level of moral development, specifically in Stage 1: Obedience and Punishment Orientation.
- Stage 1: Obedience and Punishment Orientation:
- Toddlers' decisions about right and wrong are based primarily on avoiding punishment and obtaining rewards.
- They do not yet understand the underlying reasons for rules; they simply obey to avoid negative consequences.
- Behaviors are judged as "good" or "bad" based on their immediate outcomes.
- Punishment is seen as a sign of badness, and obedience is a way to avoid it.
Nursing Insight: Behavior is motivated by reward/punishment. Discipline must be consistent, immediate, and focused on the action, not the child. Avoid shaming.
Nursing Implications for Moral Development:
- Set clear, consistent limits and consequences for behavior.
- Use positive reinforcement for desired behaviors.
- Explain rules in simple terms, focusing on the immediate impact (e.g., "Don't touch the stove, it's hot and will hurt you").
- Avoid lengthy explanations or abstract reasoning, as toddlers cannot grasp these.
- Focus on teaching simple concepts of right and wrong through consistent discipline and modeling.
1.4. Spiritual Development
Spiritual development in toddlers is largely influenced by their environment and the beliefs and practices of their primary caregivers.
- Learning through Imitation: Toddlers absorb spiritual concepts and rituals through observing and imitating their parents and family members.
- Concrete Understanding: Their understanding of spiritual concepts is very concrete and literal. Abstract ideas about God or spirituality are beyond their comprehension.
- Rituals and Routines: They may enjoy participating in religious rituals and routines, not necessarily understanding their meaning, but finding comfort and familiarity in them.
- Sense of Wonder: They have a natural sense of wonder and curiosity about the world around them, which can be a foundation for spiritual exploration later.
Nursing Insight: Spiritual understanding is concrete and imitative. Respect family's spiritual practices and accommodate rituals if they provide comfort. Avoid abstract spiritual discussions.
Nursing Implications for Spiritual Development:
- Respect the family's religious and spiritual beliefs and practices.
- Inquire about and accommodate family rituals that provide comfort (e.g., bedtime prayers).
- Recognize that spiritual development at this age is primarily observational and imitative.
- Avoid imposing religious views on families.
1.5. Development of Body Image
The development of body image in toddlers is a crucial aspect of their self-concept.
- Recognizing Self: Toddlers begin to recognize themselves as distinct from others, initially through self-recognition in mirrors and photographs.
- Labeling Body Parts: They learn to identify and name various body parts.
- Body Integrity: They have a developing, but still fragile, sense of body integrity. Minor injuries or procedures can be perceived as significant threats to their wholeness. They may believe their "insides" will fall out if they have a small cut.
- Gender Differences: They begin to recognize gender differences in body parts.
- Dress-Up and Imitation: They enjoy dressing up and imitating adult roles, which contributes to their understanding of body and self.
Nursing Implications for Development of Body Image:
- Use correct anatomical terms for body parts.
- Reassure toddlers about their body integrity during procedures or injuries.
- Allow them to explore their bodies (within appropriate boundaries) and answer their questions simply and directly.
- Minimize invasive procedures when possible, and prepare toddlers for them using age-appropriate language and visual aids.
- Encourage self-care activities like dressing and undressing to foster body awareness.
1.6. Development of Gender Identity
Gender identity, the inner sense of being male or female, begins to develop during toddlerhood.
- Awareness of Gender: Toddlers become aware of their own gender and that of others.
- Gender-Typed Play: They begin to engage in gender-typed play, often imitating the roles of same-sex adults.
- Labeling Gender: They can correctly label themselves and others as "boy" or "girl."
- Parental Influence: Parental attitudes and societal expectations heavily influence the development of gender identity.
Nursing Implications for Development of Gender Identity:
- Avoid gender stereotypes in play and language, allowing children to explore various interests.
- Support parents in fostering a positive self-image regardless of gender.
- Recognize that variations in gender expression are normal, and provide a supportive environment.
- Use inclusive language.
1.7. Social Development (Erikson: Autonomy vs. Shame and Doubt)
According to Erikson, toddlerhood is characterized by the psychosocial crisis of autonomy versus shame and doubt.
- Autonomy: Toddlers strive for independence and control over their own bodies and environment. They want to do things for themselves (e.g., feed themselves, dress themselves). This is expressed through their frequent use of "no!" and desire for choices.
- Shame and Doubt: If toddlers are consistently shamed, ridiculed, or overcontrolled when attempting to exert autonomy, they may develop feelings of shame and doubt about their abilities and sense of self-worth.
- Differentiation of Self from Others: Toddlers are increasingly aware of themselves as separate individuals.
- Social Interactions:
- Parallel Play: Toddlers typically engage in parallel play, playing alongside other children but not directly interacting with them. They may observe each other but are largely self-focused.
- Imitation: They love to imitate the actions of adults and older children.
- Brief Cooperative Play: Towards the end of toddlerhood, brief episodes of cooperative play may emerge.
- Separation Anxiety: While typically less intense than in infancy, separation anxiety can still occur, especially in unfamiliar situations.
- Stranger Anxiety: Also less pronounced but can still be present.
- Negativism: A characteristic behavior where toddlers frequently say "no" or refuse to comply, as a way to assert their developing autonomy.
- Ritualism: The need for sameness, routine, and predictability. This provides a sense of security and control in a rapidly changing world. Deviations from rituals can cause distress.
- Possessiveness: Toddlers often have a strong sense of ownership over their toys and possessions and may have difficulty sharing.
Nursing Implications for Social Development:
- Provide opportunities for toddlers to make simple choices (e.g., "Do you want to wear the red shirt or the blue shirt?").
- Encourage self-feeding and other self-care activities.
- Set clear, consistent limits to provide a sense of security and structure, but allow for exploration within those limits.
- Avoid shaming or ridiculing attempts at independence.
- Facilitate parallel play opportunities.
- Prepare toddlers for changes in routine, and try to maintain established rituals when possible (e.g., bringing a favorite blanket to the hospital).
- Teach sharing, but understand that it is a developing concept.
- Reassure parents that negativism is a normal phase of development and not defiance.
Nursing Insight: Autonomy vs. Shame and Doubt is core conflict. Offer limited, safe choices to foster independence. Avoid power struggles; allow them to do things for themselves.
Growth and Development in Toddlers
Temperament
Temperament refers to an individual's innate behavioral style and emotional characteristics. It influences how a toddler interacts with their environment and responds to various stimuli.
While not modifiable, understanding a toddler's temperament helps parents and caregivers adapt their parenting strategies.
Thomas and Chess identified nine characteristics of temperament, often grouped into three broad categories:
- Easy Child: Generally positive mood, adaptable, low or moderate intensity of reactions, regular and predictable biological rhythms. They adapt easily to new situations.
- Difficult Child: Irregular biological rhythms, negative mood, intense reactions, slow to adapt to new situations, and often withdraw from novel stimuli. They tend to be more challenging to parent.
- Slow-to-Warm-Up Child: Low activity level, generally negative mood, low intensity of reactions, adapt slowly to new situations, and may initially withdraw but eventually adapt if given time.
Nine Characteristics of Temperament (Thomas & Chess):
- Activity Level: Degree of physical motion during activity (e.g., high-energy vs. quiet).
- Rhythmicity (Regularity): Predictability of biological functions like hunger, sleep, and elimination.
- Approach/Withdrawal: Initial response to new stimuli, people, or places (e.g., immediate engagement vs. hesitation).
- Adaptability: Ease with which a child adjusts to changes in routine or environment.
- Intensity of Reaction: Energy level of response, whether positive or negative (e.g., loud laughter vs. quiet smile).
- Threshold of Responsiveness: Intensity of stimulation required to evoke a response.
- Quality of Mood: Predominant emotional state (e.g., cheerful vs. serious).
- Distractibility: Ease with which external stimuli can interfere with ongoing behavior.
- Attention Span and Persistence: Length of time an activity is pursued and ability to continue in the face of obstacles.
Nursing Implications for Temperament:
- Assess the toddler's temperament characteristics during health visits.
- Educate parents about temperament as an innate trait, not a reflection of their parenting skills or the child's "badness."
- Help parents understand their child's unique temperament and how to adapt their parenting style to promote a "goodness of fit" between parent and child.
- Suggest strategies for managing challenging temperaments (e.g., for a difficult child, maintain consistent routines, introduce new situations slowly; for a slow-to-warm-up child, allow time for adjustment).
- Validate parental feelings and offer support.
Coping With Concerns Related To Normal Growth And Development
- Toddlerhood is a period filled with developmental "tasks" that can present challenges for both the child and the parents.
- Nurses can provide valuable guidance and strategies for coping with these normal, yet sometimes frustrating, behaviors.
1.1. Toilet Training
Toilet training is a significant developmental milestone influenced by physical and psychological readiness.
- Readiness Signs (usually between 18-30 months):
- Physical Readiness:
- Ability to walk, sit, and squat.
- Has dry periods of at least 2 hours or wakes dry from a nap.
- Has regular, predictable bowel movements.
- Can pull pants up and down.
- Cognitive Readiness:
- Can understand and follow simple directions.
- Can communicate the need to go to the bathroom (verbally or nonverbally).
- Shows curiosity about using the toilet.
- Psychological Readiness:
- Expresses a desire for independence and control.
- Shows interest in the toilet and wants to imitate adults.
- Is not in a period of major stress or transition (e.g., new sibling, moving).
- Has a positive relationship with the parent.
- Physical Readiness:
Nursing Insight: Readiness, not age, is key. Educate parents on physical, cognitive, and psychological readiness cues. Starting too early causes frustration and delay.

- Nursing Interventions/Guidance:
- Patience and Positive Reinforcement: Emphasize patience, consistency, and a positive approach. Praise efforts, not just success.
- Avoid Punishment: Never punish for accidents. This can lead to fear, shame, and delayed training.
- "Readiness" Approach: Stress that training should begin when the child shows readiness, not when the parents are ready or when the child reaches a certain age.
- Equipment: Suggest a child-sized potty chair or a toilet seat insert with a step stool.
- Routine: Establish a consistent routine, such as taking the child to the potty after meals or upon waking.
- Dress: Suggest easily removable clothing.
- Bowel Training First: Often, bowel control is achieved before bladder control. Focus on one at a time.
- Nighttime Training: Nighttime bladder control usually develops after daytime control.
- Dealing with Resistance: If the child resists, stop training for a few weeks and then try again.
- Hygiene: Teach proper wiping and handwashing.
1.2. Sibling Rivalry
Sibling rivalry is a common phenomenon when a new baby enters the family, or even between existing siblings.
- Causes: Competition for parental attention, perceived loss of parental love, jealousy, and developmental stage (egocentricity).
- Manifestations: Regression (e.g., bedwetting, thumb-sucking), aggression towards the sibling, increased negativism, attention-seeking behaviors.
- Nursing Interventions/Guidance:
- Prepare the Toddler: Prepare the toddler for the new baby's arrival well in advance, involving them in preparations.
- Assure Love and Attention: Reassure the toddler of continued love and attention.
- Special Time: Dedicate special one-on-one time with the toddler each day.
- Involve the Toddler: Involve the toddler in the care of the new baby (e.g., fetching diapers, singing songs, helping with feeding).
- Avoid Comparisons: Do not compare siblings.
- Acknowledge Feelings: Validate the toddler's feelings of frustration or anger.
- Manage Aggression: Set clear limits on aggressive behavior.
- Encourage Play: Encourage positive interactions and parallel play.
- Gifts: Present a "gift" from the new baby to the toddler.
1.3. Temper Tantrums
Temper tantrums are common in toddlers and are a normal part of their development, reflecting their struggle between their desire for independence and their limited communication skills and impulse control.
- Causes: Frustration, inability to communicate needs/desires effectively, fatigue, hunger, overstimulation, desire for control/autonomy.
- Manifestations: Crying, screaming, hitting, kicking, throwing objects, breath-holding spells (less common but can occur).
- Nursing Interventions/Guidance:
- Prevention:
- Avoid situations likely to provoke tantrums (e.g., overtired, hungry).
- Offer choices (within limits) to give a sense of control.
- Prepare toddlers for transitions.
- Distraction.
- During a Tantrum:
- Remain Calm: Parents should remain calm and avoid escalating the situation.
- Ignore the Behavior (if safe): If the tantrum is for attention, ignore the behavior as long as the child is safe.
- Time-Out: Use a brief time-out (1 minute per year of age) for destructive or aggressive behavior.
- Safety First: Ensure the child is safe from injury.
- Avoid Arguing/Reasoning: Reasoning during a tantrum is ineffective.
- After a Tantrum:
- Offer comfort once the child has calmed down.
- Discuss the situation briefly and calmly, reinforcing rules.
- Return to normal activity.
- Consistency: Consistent responses from caregivers are key.
- Prevention:
1.4. Negativism
Negativism, characterized by a frequent "no" and resistance to suggestions, is a hallmark of toddlerhood.
- Causes: A natural expression of the toddler's developing autonomy and desire for independence. It's their way of asserting control.
- Manifestations: Saying "no" to everything, refusing to cooperate, doing the opposite of what is asked.
- Nursing Interventions/Guidance:
- Offer Choices: Give toddlers choices that are acceptable to the parent (e.g., "Do you want to wear the blue shirt or the red shirt?" instead of "Put on your shirt").
- Avoid "No" Questions: Phrase requests positively (e.g., "It's time to clean up" instead of "Do you want to clean up?").
- Limit Settings: Set clear and consistent limits to provide structure and security.
- Positive Reinforcement: Praise cooperative behavior.
- Humor and Playfulness: Sometimes, a playful approach can diffuse negativism.
- Patience: Remind parents that this is a normal developmental phase that will pass.
Nursing Insight: "No" is assertion of autonomy. Offer limited choices such as "Do you want the red or blue shirt?" and phrase requests positively to give a sense of control.
1.5. Stress
Toddlers can experience stress, even though they may not be able to articulate it. Significant changes or events can be stressful.
- Stressors: New sibling, moving, parental conflict/divorce, hospitalization, starting childcare, loss of a loved one, significant changes in routine.
- Manifestations: Regression, changes in sleep/eating patterns, increased irritability, clinginess, increased aggression, withdrawal, difficulty with toilet training.
- Nursing Interventions/Guidance:
- Maintain Routine: Whenever possible, maintain consistent routines.
- Predictability: Provide predictability and preparation for changes.
- Reassurance: Offer extra comfort, cuddles, and reassurance.
- Verbalize Feelings: Help the child verbalize feelings (e.g., "You seem sad").
- Play Therapy: Encourage play as a way for the child to express and process stress.
- Parental Support: Support parents in managing their own stress, as parental stress can affect the child.
- Professional Help: Recommend professional help if stress is severe or prolonged.
1.6. Regression
Regression is a temporary return to an earlier developmental stage in response to stress, illness, or changes in routine.
- Causes: New baby, hospitalization, illness, starting a new daycare, toilet training pressure, family conflict.
- Manifestations: Resuming behaviors like thumb-sucking, bedwetting (after being trained), wanting a bottle, increased clinginess, baby talk.
- Nursing Interventions/Guidance:
- Acknowledge and Validate: Acknowledge that the behavior is a normal response to stress.
- Avoid Punishment: Do not punish or shame the child for regressing.
- Provide Reassurance: Offer extra comfort and security.
- Focus on Underlying Cause: Address the underlying stressor if possible.
- Reinforce Age-Appropriate Behaviors: Gently encourage and praise age-appropriate behaviors when the stress subsides.
- Temporary Nature: Reassure parents that regression is usually temporary.
- Gradual Return: Expect a gradual return to previous developmental achievements.
Nursing Insight: Regression is a normal coping mechanism. Do not punish regressive behaviors. Provide extra comfort, address the underlying stressor, and gently encourage age-appropriate behaviors when the stress subsides.
