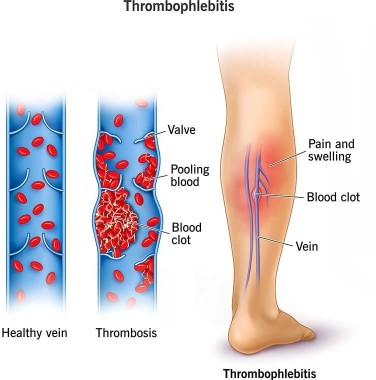
A nurse is caring for a client who is 1 day postpartum following a cesarean birth. To prevent thrombophlebitis, the nurse should contribute which of the following interventions to the client's plan of care?
Apply warm, moist soaks to the client's lower legs.
Have the client ambulate frequently in the hallway.
Keep the client on bed rest.
Place pillows under the client's knees while she is resting in bed.
The Correct Answer is B
Choice A reason: Apply warm, moist soaks to the client's lower legs is incorrect, as this action is not effective for preventing thrombophlebitis. Warm, moist soaks can provide comfort and reduce inflammation, but they do not improve blood circulation or prevent clot formation.
Choice B reason: Have the client ambulate frequently in the hallway is correct, as this action can prevent thrombophlebitis by improving venous return and preventing stasis. The nurse should encourage and assist the client to ambulate early and frequently after a cesarean birth, as long as there are no contraindications. The nurse should also monitor the client for signs of orthostatic hypotension and provide support as needed.
Choice C reason: Keep the client on bed rest is incorrect, as this action can increase the risk of thrombophlebitis by reducing blood flow and promoting stasis. Bed rest can also delay wound healing and increase the risk of infection and deconditioning. The nurse should avoid keeping the client on bed rest unless absolutely necessary.
Choice D reason: Place pillows under the client's knees while she is resting in bed is incorrect, as this action can impair blood circulation and increase the risk of thrombophlebitis. Placing pillows under the knees can cause pressure on the popliteal veins and reduce venous return. The nurse should advise the client to avoid crossing their legs or placing pillows under their knees while resting in bed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason:
Bloody show from the vagina is incorrect, as this finding is normal and expected in the second stage of labor. Bloody show refers to the passage of mucus and blood from the cervix, which indicates cervical dilation and effacement.
Choice B reason:
Early decelerations in the FHR is incorrect, as this finding is normal and benign in the second stage of labor. Early decelerations are symmetrical decreases in the FHR that mirror the contractions, which indicate fetal head compression and vagal stimulation. The nurse should continue to monitor the FHR and document the findings.
Choice C reason:
Pelvic pressure with contractions is incorrect, as this finding is normal and expected in the second stage of labor. Pelvic pressure indicates that the fetus is descending into the birth canal and that the client is ready to push.
Choice D reason:
Uterine contraction lasting 2 min is correct, as this finding is abnormal and potentially dangerous in any stage of labor. Uterine contraction lasting 2 min can indicate uterine tetany or hyperstimulation, which can cause fetal distress, placental abruption, uterine rupture, or maternal hemorrhage. The nurse should report this finding to the provider immediately and prepare to intervene as ordered.

Correct Answer is A
Explanation
Choice A reason: This is the most appropriate response because it reassures the client that the amount of lochia she passed is normal and expected after lying down for a long time. Lochia is the vaginal discharge that occurs after childbirth, consisting of blood, mucus, and uterine tissue. It usually decreases in amount and changes in color over time, from red to pink to brown to yellow.
Choice B reason: This is an incorrect response because it implies that the client has a complication that requires further evaluation. Retained placental fragments can cause excessive bleeding, infection, and uterine atony. The nurse should not alarm the client with this possibility without evidence.
Choice C reason: This is an incorrect response because it contradicts the normal patern of lochia. The amount of lochia usually decreases during the postpartum period, not increases. If the client has an increase in lochia, it could indicate a problem such as infection, subinvolution, or hemorrhage.
Choice D reason: This is an incorrect response because it confuses the client with unrelated information. Urinary tract infections are not associated with increased lochia. They are caused by bacteria entering the urinary tract and can cause symptoms such as dysuria, frequency, urgency, and hematuria. The nurse should not suggest that the client has a urinary tract infection without evidence.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today