A nurse is preparing to administer dinoprostone gel to a client who is pregnant. The client asks the nurse about the purpose of the medication. Which of the following responses should the nurse make?
Dinoprostone stimulates uterine contractions.
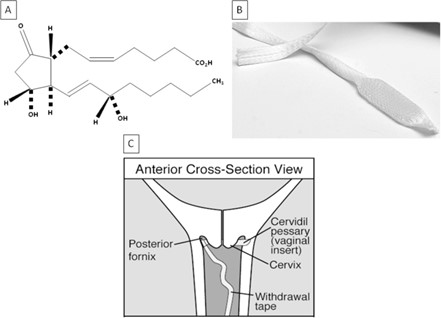
Dinoprostone promotes softening of the cervix.
Dinoprostone relaxes uterine contractions.
Dinoprostone assists with ending the pregnancy.
The Correct Answer is B
Choice A reason:
Dinoprostone stimulates uterine contractions is incorrect, as this is not the primary purpose of the medication. Dinoprostone is a prostaglandin that can induce labor by ripening the cervix and enhancing uterine contractility, but it is not used solely for stimulating contractions.
Choice B reason:
Dinoprostone promotes softening of the cervix is correct, as this is the main purpose of the medication. Dinoprostone is used to prepare the cervix for labor by increasing its softness, dilation, and effacement. This can facilitate the descent of the fetus and shorten the duration of labor.
Choice C reason:
Dinoprostone relaxes uterine contractions is incorrect, as this is the opposite effect of the medication. Dinoprostone can increase uterine tone and frequency, which can help initiate or augment labor. The nurse should monitor the client for signs of uterine hyperstimulation or fetal distress.
Choice D reason:
Dinoprostone assists with ending the pregnancy is incorrect, as this is not the intended use of the medication. Dinoprostone can be used to terminate a pregnancy in some cases, such as fetal demise or missed abortion, but it is not routinely used for this purpose. The nurse should explain to the client that dinoprostone is used to induce labor and not to end a pregnancy.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
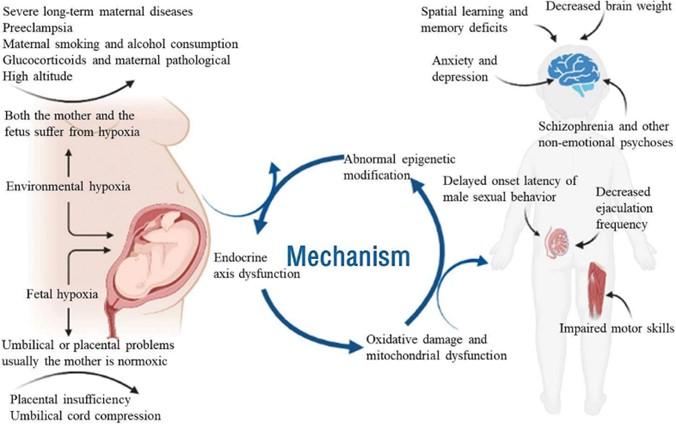
Choice A reason: Position the client on her side is correct, as this is the first action the nurse should take according to the ABCDE priority framework. Late decelerations are symmetrical decreases in the fetal heart rate that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency and fetal hypoxia. Positioning the client on her side can improve blood flow and oxygen delivery to the placenta and fetus by relieving pressure on the vena cava and aorta.
Choice B reason: Elevate the client's legs is incorrect, as this is not a priority action for a client who has late decelerations. Elevating the legs can increase venous return and cardiac output, but it can also reduce blood flow and oxygen delivery to the placenta and fetus by compressing the vena cava and aorta.
Choice C reason: Administer oxygen via face mask is incorrect, as this is not the first action the nurse should take, although it is important to do later. Administering oxygen can increase oxygen saturation and delivery to the placenta and fetus, but it does not address the cause of uteroplacental insufficiency or improve blood flow.
Choice D reason: Increase the infusion rate of the IV fluid is incorrect, as this is not the first action the nurse should take, although it may be indicated later. Increasing the infusion rate of IV fluid can expand blood volume and improve placental perfusion, but it does not address the cause of uteroplacental insufficiency or improve blood flow. The nurse should obtain a provider's order before increasing the IV fluid rate.
Correct Answer is B
Explanation
Choice A reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm above the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
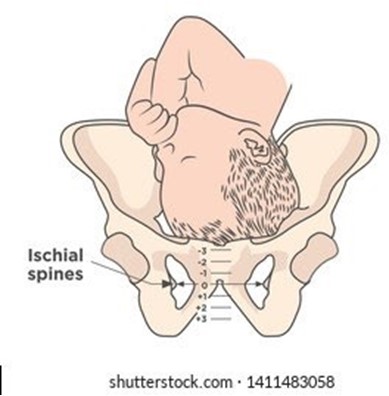
Choice B reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines is correct, as this follows the correct order and measurement of cervical assessment. Cervical dilation, effacement, and station are recorded in that order to describe the progress of labor. Station refers to the relationship between the presenting part of the fetus and the maternal pelvis, measured by the level of the ischial spines. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Choice C reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
Choice D reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not match the documentation of station. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today