A nurse is reinforcing teaching of a female client who has a family history of type 2 diabetes mellitus. The nurse should include which of the following risk factors for developing type 2 diabetes mellitus in the teaching?
Sedentary lifestyle
Triglyceride level of 100 mg/dL
Blood glucose of 98 mg/dL
Recent viral infection
The Correct Answer is A
Choice A: Sedentary lifestyle. This is a risk factor for developing type 2 diabetes mellitus, which is a condition that occurs when the body becomes resistant to the action of insulin or does not produce enough insulin to maintain normal blood glucose levels. Insulin is a hormone that helps glucose enter the cells and be used for energy. A sedentary lifestyle can increase the risk of type 2 diabetes mellitus by reducing physical activity, which can improve insulin sensitivity and lower blood glucose levels.
Choice B: Triglyceride level of 100 mg/dL. This is not a risk factor for developing type 2 diabetes mellitus, but rather a normal value. Triglycerides are a type of fat that circulates in the blood and can be used for energy or stored in adipose tissue. A high triglyceride level can indicate an increased risk of cardiovascular disease, but it is not directly related to type 2 diabetes mellitus.
Choice C: Blood glucose of 98 mg/dL. This is not a risk factor for developing type 2 diabetes mellitus, but rather a normal value. Blood glucose is the amount of glucose in the blood, which can vary depending on food intake, physical activity, and hormonal regulation. A high blood glucose level can indicate type 2 diabetes mellitus, but it is not a cause of it.
Choice D: Recent viral infection. This is not a risk factor for developing type 2 diabetes mellitus, but rather a possible trigger for type 1 diabetes mellitus, which is a condition that occurs when the immune system destroys the beta cells of the pancreas that produce insulin. A viral infection can trigger an autoimmune response that attacks the beta cells and causes type 1 diabetes mellitus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Notify the nurse manager. This is an important action that the nurse should take, but not a priority. The nurse should notify the nurse manager to report the error and seek guidance on how to proceed. The nurse manager can also provide support and feedback to the nurse and help prevent similar errors in the future.
Choice B: Give the client 15 to 20 g of carbohydrate. This is a necessary action that the nurse should take, but not the priority. The nurse should give the client 15 to 20 g of carbohydrates to raise their blood glucose level and prevent or treat hypoglycemia. The nurse should choose a fast-acting carbohydrate source, such as juice, glucose tablets, or candy.
Choice C: Complete an incident report. This is a required action that the nurse should take, but not the priority. The nurse should complete an incident report to document the error and its consequences. The incident report can help identify the root cause of the error and improve patient safety and quality of care.
Choice D: Check the client’s blood glucose level. This is the priority action that the nurse should identify according to the ABCDE principle, which prioritizes interventions based on airway, breathing, circulation, disability, and exposure. The nurse should check the client’s blood glucose level to confirm the error and assess the risk of hypoglycemia, which is a low level of glucose in the blood. Hypoglycemia can cause symptoms such as sweating, trembling, confusion, and loss of consciousness. It can be life-threatening if not treated promptly.
Correct Answer is A
Explanation
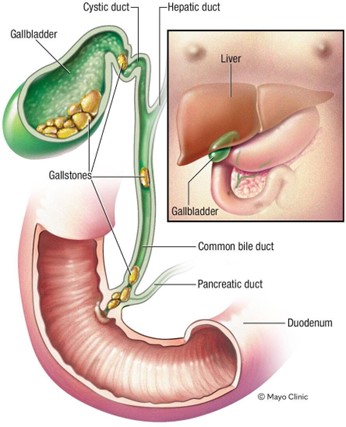
Choice A: Faty stools. This is a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis, which is the presence of gallstones in the gallbladder or bile ducts. The common bile duct carries bile from the liver and gallbladder to the duodenum, where it helps digest fats. If the common bile duct is obstructed by a gallstone, bile cannot reach the duodenum and fats cannot be properly absorbed. This results in fatty stools, which are also known as steatorrhea. Fatty stools are pale, bulky, greasy, and foul-smelling.
Choice B: Ecchymosis of the extremities. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Ecchymosis of the extremities is a sign of bleeding under the skin, which can be caused by trauma, coagulation disorders, or medications. It is not related to bile duct obstruction or gallstones.
Choice C: Straw-colored urine. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Straw-coloured urine is a normal colour of urine, which indicates adequate hydration and kidney function. It is not affected by bile duct obstruction or gallstones.
Choice D: Tenderness in the left upper abdomen. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Tenderness in the left upper abdomen is a sign of splenomegaly, which is an enlargement of the spleen due to infection, inflammation, or cancer. It is not related to bile duct obstruction or gallstones.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today