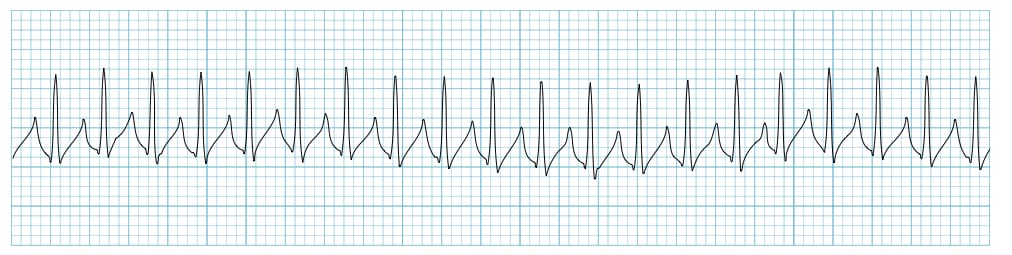
An adult client is being admitted to the coronary care unit with a possible myocardial infarction (MI). The client reports feeling like they are going to "pass out." The cardiac monitor displays the rhythm shown. The client's respiratory rate is 12 to 16 breaths/minute and blood pressure is 78/52 mm Hg. The nurse auscultates clear breath sounds bilaterally and the skin is pale and diaphoretic. After administering oxygen, which action should the nurse prepare to perform?
Assist the client to perform vagal maneuver or bear down.
Give an anticholinergic medication.
Administer a sedative and cardiovert the client.
Give a beta blocker medication.
The Correct Answer is C
Rationale:
A. Assist the client to perform vagal maneuver or bear down: The ECG shows supraventricular tachycardia (SVT) with a very rapid, regular rhythm. While vagal maneuvers may help slow the rate in stable clients, this client’s hypotension (78/52 mm Hg) and presyncope indicate instability.
B. Give an anticholinergic medication: Anticholinergic agents like atropine are used for bradyarrhythmias, not for tachycardia. Administering such a drug would further increase the heart rate and worsen myocardial oxygen demand in this client with suspected myocardial infarction.
C. Administer a sedative and cardiovert the client: The rhythm and symptoms indicate unstable supraventricular tachycardia. Synchronized cardioversion is the immediate treatment for unstable tachyarrhythmias with a pulse to restore sinus rhythm and improve perfusion. Sedation is given beforehand if the client is conscious.
D. Give a beta blocker medication: Beta blockers are appropriate for stable tachyarrhythmias but can dangerously lower blood pressure in an unstable patient. The client’s hypotension and near-syncope require electrical rather than pharmacologic intervention.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Rationale:
A. Skeletal traction misalignment: While misalignment can cause discomfort and complications in spinal cord injury clients, it is not the most common or immediate trigger of autonomic dysreflexia. Assessment of alignment is secondary to more urgent causes of sympathetic overactivity.
B. Profuse forehead diaphoresis: Sweating is a symptom of autonomic dysreflexia but is a manifestation rather than a precipitating factor. Identifying the cause of the dysreflexia takes priority over treating symptoms alone.
C. An acutely distended bladder: Bladder distension is the most common precipitating factor for autonomic dysreflexia in clients with lesions at T6 or above. Immediate assessment and relief of urinary retention are critical to prevent severe hypertension, stroke, or other life-threatening complications.
D. A severe pounding headache: Headache is a classic symptom of autonomic dysreflexia, reflecting elevated blood pressure. While important to recognize, it indicates the presence of the condition rather than identifying the cause that must be addressed first.
Correct Answer is ["B","C","E"]
Explanation
Rationale:
A. Increase the fraction of inspired oxygen: Increasing FiO₂ is only necessary if the client shows signs of hypoxemia or respiratory distress. Since oxygen saturation and respiratory status are not reported as compromised, this is not the immediate intervention.
B. Gather supplies for extubation: The client has been weaned to 0 cm H₂O pressure support, indicating readiness for spontaneous breathing. Preparing extubation supplies ensures the nurse is ready for safe removal of the endotracheal tube when the healthcare provider decides it is appropriate.
C. Set up supplemental oxygen delivery: After extubation, the client may require supplemental oxygen to maintain adequate oxygenation. Setting up oxygen delivery devices in advance promotes a smooth transition from mechanical ventilation to spontaneous breathing.
D. Offer the client ice chips: Ice chips are inappropriate for an intubated client or a client being evaluated for extubation, as swallowing may be impaired and aspiration risk is high. Oral intake should only be introduced after a swallow assessment.
E. Set the ventilator to give mandatory breaths: Providing mandatory breaths may be necessary if the client shows signs of respiratory fatigue or inadequate ventilation. This intervention supports the client temporarily until extubation is safely performed.
F. Suggest a different ventilator mode to the provider: While input may be valuable, the healthcare provider evaluates ventilator management and decides on mode adjustments. The nurse should focus on preparing for extubation and supporting spontaneous breathing.
G. Place a nasogastric tube: NG tube insertion is not indicated solely because the client is being weaned from the ventilator. This intervention is unrelated unless there are concerns about gastric distention or feeding tolerance post-extubation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today