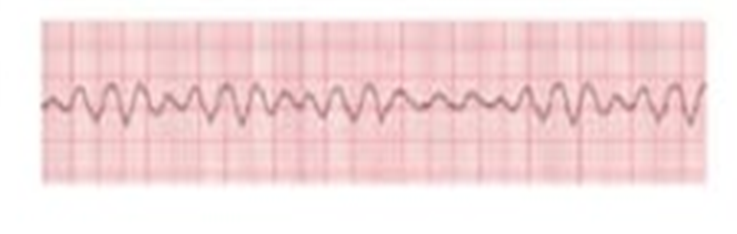
During a code blue, the nurse observes the following rhythm on the monitor (see below or in the attachment of a 6 second rhythm strip) following a defibrillation shock. What is the nurses' first action?
Assess the patient's blood pressure
Set the pacer to 65 beats per minute
Start chest compressions
Prepare for cardioversion
The Correct Answer is C
A. Assess the patient's blood pressure: In ventricular fibrillation, the patient is pulseless and unresponsive, so assessing blood pressure will not provide meaningful information. Immediate life-saving interventions take priority over vital sign assessment.
B. Set the pacer to 65 beats per minute: Pacing is used for bradyarrhythmias with a perfusing rhythm, not for pulseless ventricular fibrillation. It cannot establish effective cardiac output in a chaotic ventricular rhythm.
C. Start chest compressions: After a defibrillation shock, if the patient remains in pulseless VF, high-quality CPR should be initiated immediately to maintain circulation to vital organs. Early chest compressions are critical for increasing the chances of return of spontaneous circulation (ROSC) and improving outcomes.
D. Prepare for cardioversion: Synchronized cardioversion is used for unstable rhythms with a pulse, such as atrial fibrillation or VT with a pulse. In pulseless VF, unsynchronized defibrillation and CPR are required, not cardioversion.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. Teach the patient to use a soft bristled toothbrush: This teaching is appropriate for patients receiving anticoagulation therapy to reduce bleeding risk. However, it does not address the urgent clinical concern of recurrent pulmonary embolism while already on anticoagulants, which suggests possible treatment failure, nonadherence, drug interactions, or incorrect dosing.
B. Instruct the patient to eliminate vitamin K from the diet: For patients taking warfarin, vitamin K intake should remain consistent rather than eliminated. Complete avoidance can destabilize anticoagulation control and increase INR variability. Additionally, this intervention does not directly address why a second PE occurred despite therapy.
C. Perform a medication reconciliation: A recurrent PE while on anticoagulation raises concern for nonadherence, incorrect dosing, drug–drug interactions, or subtherapeutic anticoagulation levels. Medication reconciliation helps identify discrepancies, missed doses, or interactions that may have reduced anticoagulant effectiveness and is a priority safety action.
D. Refer the patient to a chronic illness support group: Psychosocial support may be beneficial long term, but it does not address the immediate clinical issue of recurrent thromboembolism. The priority is to determine why anticoagulation therapy failed and prevent further potentially life-threatening embolic events.
Correct Answer is D
Explanation
A. Reinsert the tube into the chest tube insertion site: Reinserting a chest tube that has become dislodged is outside the scope of nursing practice and risks introducing infection and causing further trauma. Re-insertion must be performed by a qualified provider using sterile technique under appropriate conditions.
B. Insert the end of the chest tube in a container of sterile water: Placing the end of a dislodged chest tube into sterile water is appropriate only if the tube has disconnected from the drainage system but remains in the patient’s chest. In this scenario, the tube is lying on the floor, indicating it has been removed from the patient, so this action is not appropriate.
C. Auscultate the lung sounds in bilateral lung fields: Assessing lung sounds is important, but it is not the first priority. When a chest tube becomes dislodged from the patient, there is an immediate risk of air entering the pleural space and causing a tension pneumothorax. The insertion site must be addressed before further assessment.
D. Apply a sterile dressing to the chest tube insertion site: The priority is to immediately cover the insertion site with a sterile occlusive dressing (often taped on three sides) to prevent air from entering the pleural cavity and causing a life-threatening tension pneumothorax. This intervention directly addresses the most immediate physiological threat.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today