Provided is an ECG image of Ventricular tachycardia.
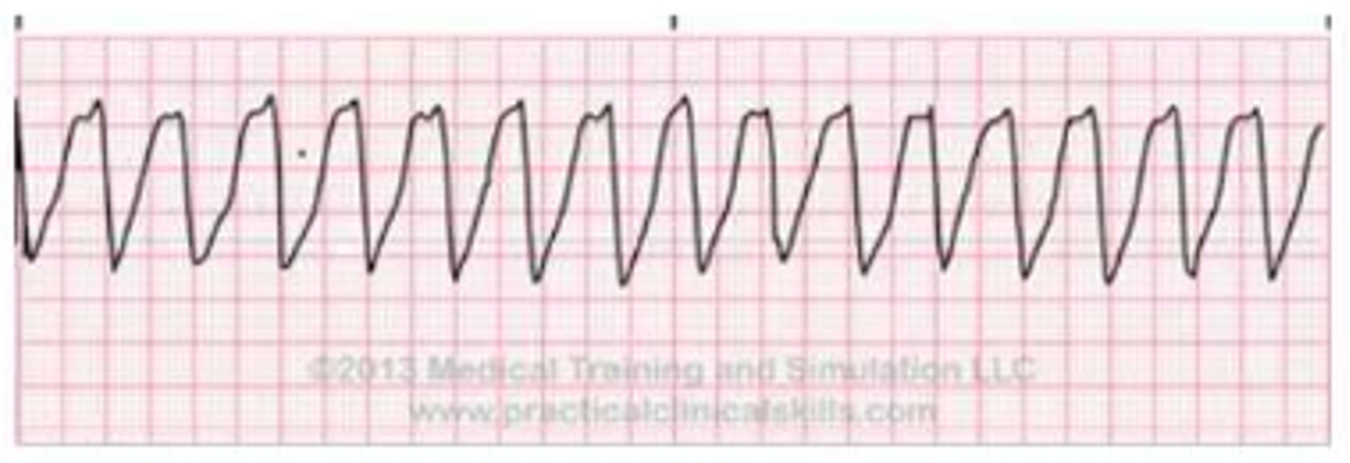
Identify the wave pattern and describe it.
Rapid, regular wide QRS complexes with no visible P waves.
Chaotic electrical activity with no identifiable QRS complexes.
Early P waves with a different shape followed by a normal QRS.
Progressive lengthening of the PR interval until a QRS is dropped.
The Correct Answer is A
Choice A rationale
Ventricular tachycardia is characterized by rapid, repetitive firing from an ectopic focus or reentrant circuit within the ventricular myocardium. Because the impulse does not follow the rapid His-Purkinje system, ventricular depolarization is slow and inefficient, resulting in QRS complexes wider than 0.12 seconds. The high rate, typically 100 to 250 beats per minute, overrides the sinus node, meaning P waves are buried or dissociated. This severely compromises cardiac output due to reduced filling time.
Choice B rationale
Chaotic electrical activity without any identifiable QRS complexes describes ventricular fibrillation. In this state, the ventricles merely quiver and do not provide any effective contraction or cardiac output. This is a pulseless rhythm that requires immediate defibrillation to restore organized activity. While ventricular tachycardia is also dangerous, it maintains organized QRS complexes, whereas fibrillation is a total loss of electrical and mechanical organization, appearing as a wavy or jagged baseline on the ECG.
Choice C rationale
Early P waves with a different shape followed by a normal QRS are known as premature atrial contractions. These occur when an irritable focus in the atrium fires before the next expected sinus impulse. The resulting QRS is usually narrow because the impulse still travels through the normal ventricular conduction system. This is a common, often benign finding and does not resemble the wide, rapid, and potentially lethal ventricular complexes seen in tachycardia.
Choice D rationale
A progressive lengthening of the PR interval until a QRS complex is dropped is the hallmark of Mobitz Type I or Wenckebach second-degree heart block. This occurs due to a delay at the atrioventricular node that worsens with each beat until conduction fails entirely for one cycle. This is an atrial-ventricular conduction issue, not a primary ventricular arrhythmia. Ventricular tachycardia does not involve PR interval cycles as the ventricles are firing independently.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A rationale
While aspirin does possess analgesic properties by inhibiting the synthesis of prostaglandins in the central and peripheral nervous systems, this is not the primary reason for its prescription following a myocardial infarction. In the context of post-MI care, the dose of 325 mg is intended for its systemic vascular benefits rather than simple pain relief. Other medications or lower doses of aspirin might be used for pain, but the clinical priority here is cardiovascular protection.
Choice B rationale
Aspirin exhibits anti-inflammatory effects by blocking cyclooxygenase enzymes, which reduces the production of mediators that cause tissue swelling and pain. Although inflammation plays a significant role in the progression of atherosclerosis, the specific indication for a client with a history of myocardial infarction focuses more on the immediate prevention of acute thrombotic events. While the anti-inflammatory benefit is present, it is secondary to the critical need for maintaining patency in the coronary arteries.
Choice C rationale
The antipyretic action of aspirin involves acting on the hypothalamus to override an interleukin-induced increase in body temperature. While effective for reducing fever, this pharmacological action is irrelevant to the long-term management of a client with a history of myocardial infarction. Clients in this category are not typically suffering from chronic febrile conditions; therefore, using aspirin for its heat-reducing properties would not provide the specific secondary prevention required for their underlying cardiac pathology.
Choice D rationale
In post-myocardial infarction management, aspirin is primarily used for its antiplatelet aggregate effect. It irreversibly inhibits the cyclooxygenase-1 enzyme within platelets, preventing the formation of thromboxane A2, which is a potent inducer of platelet aggregation. By reducing the ability of platelets to clump together, aspirin decreases the risk of re-occlusion of coronary arteries and prevents subsequent ischemic events. This is the therapeutic cornerstone for long-term survival and reduction of recurrent cardiac mortality.
Correct Answer is B
Explanation
Choice A rationale
Conduction delay through the atrioventricular node typically characterizes first degree heart block rather than atrial fibrillation. In atrial fibrillation, the atrioventricular node actually acts as a gatekeeper, attempting to block the overwhelming number of electrical impulses arriving from the atria. Slowed conduction would result in a bradycardic rhythm, whereas the dizziness and palpitations described by the client are usually associated with the rapid and irregular ventricular response common in this dysrhythmia.
Choice B rationale
Atrial fibrillation involves disorganized electrical activity originating from multiple ectopic foci within the atria, bypassing the sinoatrial node. This results in rapid, chaotic impulses that cause the atria to quiver rather than contract effectively. This loss of atrial kick and the subsequent irregular ventricular rate significantly reduce cardiac output and stroke volume. The resulting decrease in cerebral perfusion leads to dizziness, while the irregular, rapid heartbeats are perceived by the client as palpitations.
Choice C rationale
A sinoatrial node firing at a rate greater than 100 beats per minute defines sinus tachycardia, which is a regular rhythm. While sinus tachycardia can cause palpitations during exercise or stress, it does not involve the chaotic atrial activity seen in fibrillation. In atrial fibrillation, the sinoatrial node is no longer the primary pacemaker. The atrial rate in fibrillation can exceed 350 to 600 impulses per minute, which is far beyond the normal physiological limits of sinus tachycardia.
Choice D rationale
An electrical signal occurring before the expected sinus impulse describes a premature atrial contraction or a premature ventricular contraction. While these ectopics can cause a sensation of a skipped beat or palpitations, they are isolated events within an otherwise stable rhythm. Atrial fibrillation is a sustained and continuous state of electrical chaos rather than a single premature beat. Therefore, isolated premature signals do not explain the persistent dizziness and ongoing palpitations associated with this specific cardiac condition.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today