The community health nurse utilizes which of the following approaches to explain the factors that allow the reproduction and spread of infectious disease?
Natural history of disease
Health promotion
Levels of prevention
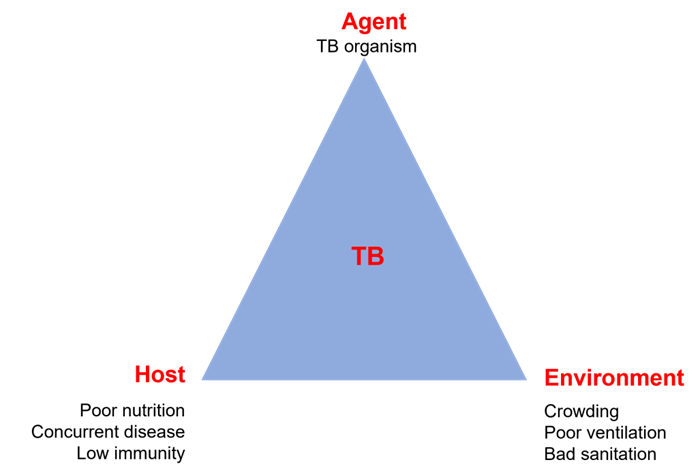
Epidemiologic triangle
The Correct Answer is D
Choice A reason: Natural history of disease is not an approach that explains the factors that allow the reproduction and spread of infectious disease. Natural history of disease is a concept that describes the progression and outcome of disease in the absence of any intervention. It includes stages such as susceptibility, exposure, incubation, prodrome, clinical, recovery, disability, or death.
Choice B reason: Health promotion is not an approach that explains the factors that allow the reproduction and spread of infectious diseases. Health promotion is a process that enables people to increase control over and improve their health. It involves strategies such as education, advocacy, policy, or community development.
Choice C reason: Levels of prevention is not an approach that explains the factors that allow the reproduction and spread of infectious disease. Levels of prevention is a framework that classifies different types of interventions based on their timing and purpose. It includes primary prevention (before disease occurs), secondary prevention (early detection and treatment), and tertiary prevention (reducing complications and disabilities).
Choice D reason: Epidemiologic triangle is an approach that explains the factors that allow the reproduction and spread of infectious disease. Epidemiologic triangle is a model that identifies three essential components of an infectious disease: agent (the microorganism that causes the disease), host (the person or animal that is infected), and environment (the physical, biological, or social factors that influence the transmission). The interaction and balance among these components determine the occurrence and spread of an infectious disease.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Hypertension is a manifestation of increased intracranial pressure, as it reflects the body's attempt to maintain adequate cerebral perfusion pressure (CPP) and blood flow to the brain. CPP is the difference between the mean arterial pressure (MAP) and the intracranial pressure (ICP). When ICP rises, MAP must also rise to keep CPP constant and prevent cerebral ischemia. Hypertension is part of the Cushing's triad, which is a classic sign of increased ICP that also includes bradycardia and irregular respirations.
Choice B reason: Tinnitus is not a manifestation of increased intracranial pressure, as it does not affect the auditory system. Tinnitus is a ringing, buzzing, or hissing sound in the ears that can be caused by various factors, such as ear infections, noise exposure, medications, or aging. Tinnitus may be associated with other neurological conditions, such as Meniere's disease, acoustic neuroma, or multiple sclerosis, but not with increased ICP.
Choice C reason: Hypotension is not a manifestation of increased intracranial pressure, as it indicates a decrease in MAP and CPP, which can lead to cerebral ischemia and infarction. Hypotension can be caused by various factors, such as blood loss, dehydration, shock, or medications. Hypotension may worsen the outcome of increased ICP by reducing the oxygen and nutrient delivery to the brain.
Choice D reason: Tachycardia is not a manifestation of increased intracranial pressure, as it contradicts Cushing's triad. Tachycardia is an increase in heart rate that can be caused by various factors, such as anxiety, pain, fever, dehydration, or medications. Tachycardia may increase the oxygen demand and metabolic rate of the brain, which can exacerbate the effects of increased ICP.
Correct Answer is C
Explanation
Choice A reason: "Diet and exercise is good for you and good for your heart." This statement is true, but it is not the appropriate nursing response. It does not address the client's concerns or provide any specific information about cardiac rehabilitation. It may also sound dismissive or patronizing to the client.
Choice B reason: "It's not unusual to feel that way at first, but once you learn the routine, you'll enjoy it." This statement is empathetic, but it is not the appropriate nursing response. It does not explain the purpose or benefits of cardiac rehabilitation. It may also sound unrealistic or optimistic to the client.
Choice C reason: "Cardiac rehabilitation cannot undo the damage to your heart, but it can help you get back to your previous level of activity safely." This statement is the appropriate nursing response. It acknowledges the client's condition and provides factual information about cardiac rehabilitation. It also emphasizes the positive outcomes of cardiac rehabilitation, such as improving physical function, reducing symptoms, and preventing further complications.
Choice D reason: "Your doctor is the expert here, and I'm sure he would only recommend what is best for you." This statement is respectful, but it is not the appropriate nursing response. It does not answer the client's question or provide any education about cardiac rehabilitation. It may also sound evasive or deferential to the client.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today