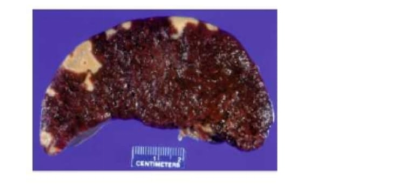
A 75-year-old woman with a recent history of myocardial infarction develops hemopericardium and expires. At autopsy. multiple wedge-shaped lesions are observed on the surface of the patient's spleen (shown). These pale infarcts were most likely caused by thromboemboli originating in which of the following anatomic locations?
Brain
Heart
Lungs
Liver
Spleen
The Correct Answer is B
A. Brain: Emboli originating in the brain would not travel systemically to the spleen. Instead, brain emboli cause localized cerebral infarctions or strokes.
B. Heart: Thromboemboli from the heart, particularly after a myocardial infarction, can arise from mural thrombi in the left ventricle. These emboli are released into the systemic arterial circulation and can lodge in end organs like the spleen, kidneys, or extremities, producing the characteristic wedge-shaped splenic infarcts seen in this patient.
C. Lungs: Pulmonary emboli originate from venous thrombi and lodge in the pulmonary arteries. They do not enter systemic circulation due to the filtering effect of the pulmonary capillary bed, so the spleen is not affected by emboli from the lungs.
D. Liver: The liver receives blood primarily via the portal vein, and thrombi here generally do not embolize to the systemic circulation. Hepatic thrombi do not cause splenic infarcts.
E. Spleen: While the infarcts are located in the spleen, they are the result of emboli lodging in splenic arteries rather than arising within the spleen itself. Therefore, the source of the thromboemboli is systemic, most commonly the heart.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Albumin:Albumin is the most abundant plasma protein and primarily maintains oncotic pressure and transports molecules. It is not a structural component of the fibrinous exudate seen in pericarditis.
B. Fibrin:Fibrin is a key plasma-derived protein formed from fibrinogen during the coagulation cascade. In fibrinous pericarditis, increased vascular permeability allows plasma proteins, particularly fibrinogen, to leak into the pericardial space, where it polymerizes into fibrin. This forms the characteristic “shaggy” or “bread-and-butter” appearance on the heart surface.
C. Fibronectin:Fibronectin is an extracellular matrix glycoprotein involved in tissue repair and cell adhesion. While it may play a minor role in wound healing, it is not the primary protein responsible for the gross fibrinous exudate in pericarditis.
D. Plasmin:Plasmin is a fibrinolytic enzyme that breaks down fibrin clots. It regulates clot dissolution but is not the structural protein forming the fibrinous exudate.
E. Thrombin:Thrombin is a protease that converts fibrinogen to fibrin during coagulation. While it initiates fibrin formation, the exudate itself is composed of fibrin polymers rather than thrombin.
Correct Answer is E
Explanation
A. Anaphylactic:Anaphylactic shock results from a severe allergic reaction, leading to widespread vasodilation, hypotension, and bronchospasm. There is typically a rapid onset following exposure to an allergen, and fever or leukocytosis is not a hallmark, making it less likely in this patient.
B. Cardiogenic:Cardiogenic shock is caused by failure of the heart to pump effectively, often due to myocardial infarction or severe arrhythmias. While hypotension and tachypnea occur, fever, leukocytosis, and evidence of infection (gram-negative organisms in urine) point toward an infectious etiology rather than primary cardiac failure.
C. Hypovolemic:Hypovolemic shock results from fluid or blood loss, leading to hypotension and tachycardia. It does not typically cause fever or leukocytosis, and there is no indication of hemorrhage in this patient, making it an unlikely explanation.
D. Neurogenic:Neurogenic shock arises from disruption of sympathetic nervous system control, often after spinal cord injury, leading to hypotension and bradycardia. Fever and leukocytosis are not characteristic, and the patient’s infection markers suggest a different etiology.
E. Septic:Septic shock is a distributive shock caused by a severe systemic infection. This patient’s hypotension, tachypnea, fever, elevated WBC count with neutrophilia, and gram-negative organisms in the urine are classic features of sepsis leading to septic shock. The clinical picture of infection-induced vasodilation and multiorgan stress makes septic shock the most likely cause.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today