A nurse is caring for a client who has a brain tumor. The client displays decorticate posturing in response to painful stimuli. Which of the following images illustrates decorticate posturing?
A
B
None
None
None
None
The Correct Answer is B
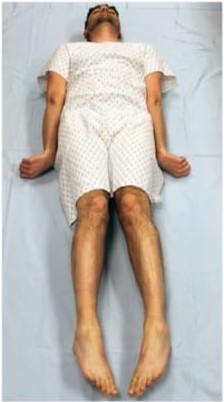
The first image illustrates decerebrate posturing (also known as extensor posturing). In this more severe posture, the arms are rigidly extended and adducted, the wrists are pronated, the fingers are flexed, and the legs are rigidly extended with plantar flexion. This is caused by damage to the brainstem at or below the red nucleus (midbrain) and indicates a worse prognosis.
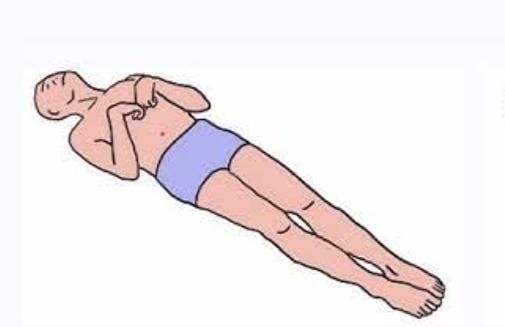
The second image illustrates decorticate posturing (also known as flexor posturing). In this posture, the client's arms are rigidly flexed and adducted (bent inward toward the chest), the fists are clenched, and the legs are extended and internally rotated. This is typically caused by damage to the corticospinal tracts above the red nucleus (above the midbrain).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. LDL: Low-density lipoprotein (LDL) is used to assess cholesterol levels and cardiovascular risk, but it does not influence warfarin therapy. Monitoring LDL is not relevant to dosing or safety of anticoagulation.
B. BUN: Blood urea nitrogen (BUN) reflects kidney function, which is important for some medications, but warfarin is metabolized by the liver, not the kidneys. BUN is not required before administering warfarin.
C. INR: The international normalized ratio (INR) measures the effectiveness of warfarin and the client’s coagulation status. Monitoring INR ensures the dose is therapeutic and reduces the risk of bleeding or clot formation in atrial fibrillation.
D. Hct: Hematocrit measures the proportion of red blood cells and helps assess anemia or blood loss, but it does not guide warfarin dosing. While low Hct may indicate bleeding, INR is the primary laboratory value to monitor before administration.
Correct Answer is D
Explanation
A. Hypocalcemia: Heat exhaustion does not typically cause low calcium levels. Calcium imbalances are more often related to parathyroid disorders, vitamin D deficiency, or certain medications rather than fluid loss from heat exposure.
B. Hyperphosphatemia: Elevated phosphate levels are not characteristic of heat exhaustion. Phosphate disturbances usually occur with kidney dysfunction or severe cellular breakdown, not from dehydration and electrolyte loss due to heat.
C. Hyperkalemia: Potassium levels may actually decrease or remain normal in heat exhaustion due to excessive sweating and fluid loss. Hyperkalemia is not a primary concern unless there is underlying renal impairment or extensive tissue damage.
D. Hypernatremia: Excessive fluid loss through sweating without adequate water replacement leads to elevated sodium levels in the blood. Hypernatremia is a common electrolyte imbalance in heat exhaustion and contributes to symptoms such as thirst, confusion, and neurologic changes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today