A nurse is discussing the importance of skin hydration with an elderly patient. Which recommendation is appropriate to enhance skin health?
Limit fluid intake to maintain skin hydration.
Applying a moisturizer immediately after bathing.
Use scented products to ensure skin safety.
Bathe in hot water for better cleanliness.
The Correct Answer is B
Choice A reason: Limiting fluid intake is counterproductive and dangerous for skin health. Adequate systemic hydration is necessary to maintain the turgor and resilience of the dermis. Older adults should be encouraged to drink sufficient water to prevent intracellular and extracellular dehydration, which directly leads to xerosis and skin fragility.
Choice B reason: Applying an emollient or moisturizer within 3 minutes of bathing is the most effective way to trap moisture in the stratum corneum. This helps to restore the skin's natural lipid barrier, which is often depleted in older adults, thereby reducing transepidermal water loss and preventing dry, itchy skin.
Choice C reason: Scented products often contain alcohols and synthetic fragrances that can act as irritants or allergens, especially for the thinning skin of an elderly patient. Fragrance-free and hypoallergenic products are recommended to minimize the risk of contact dermatitis and further drying of the skin's surface.
Choice D reason: Hot water strips the skin of its natural essential oils and can cause vasodilation that increases itching and irritation. Older adults should be advised to use lukewarm water and limit the duration of baths or showers to prevent excessive drying and potential thermal injury to their fragile skin.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Intact skin with localized, non-blanchable erythema defines a stage 1 pressure injury. At this stage, the heralding sign is skin redness that does not turn white when pressed, indicating that the inflammatory response is occurring in the dermis, but the epidermal barrier has not yet been breached or compromised by the pressure.
Choice B reason: Full-thickness skin loss with visible adipose (fat) tissue is the clinical hallmark of a stage 3 pressure injury. In stage 3, the damage extends through the epidermis and dermis into the subcutaneous layer. Slough may be present, and there may be undermining or tunneling, but deeper structures like muscle, tendon, or bone are not yet exposed.
Choice C reason: Full-thickness skin loss with visible bone, tendon, or muscle defines a stage 4 pressure injury. This is the most severe stage of localized tissue destruction, often accompanied by extensive slough or eschar. These injuries carry a high risk for osteomyelitis and require complex wound management and nutritional support to facilitate any degree of healing.
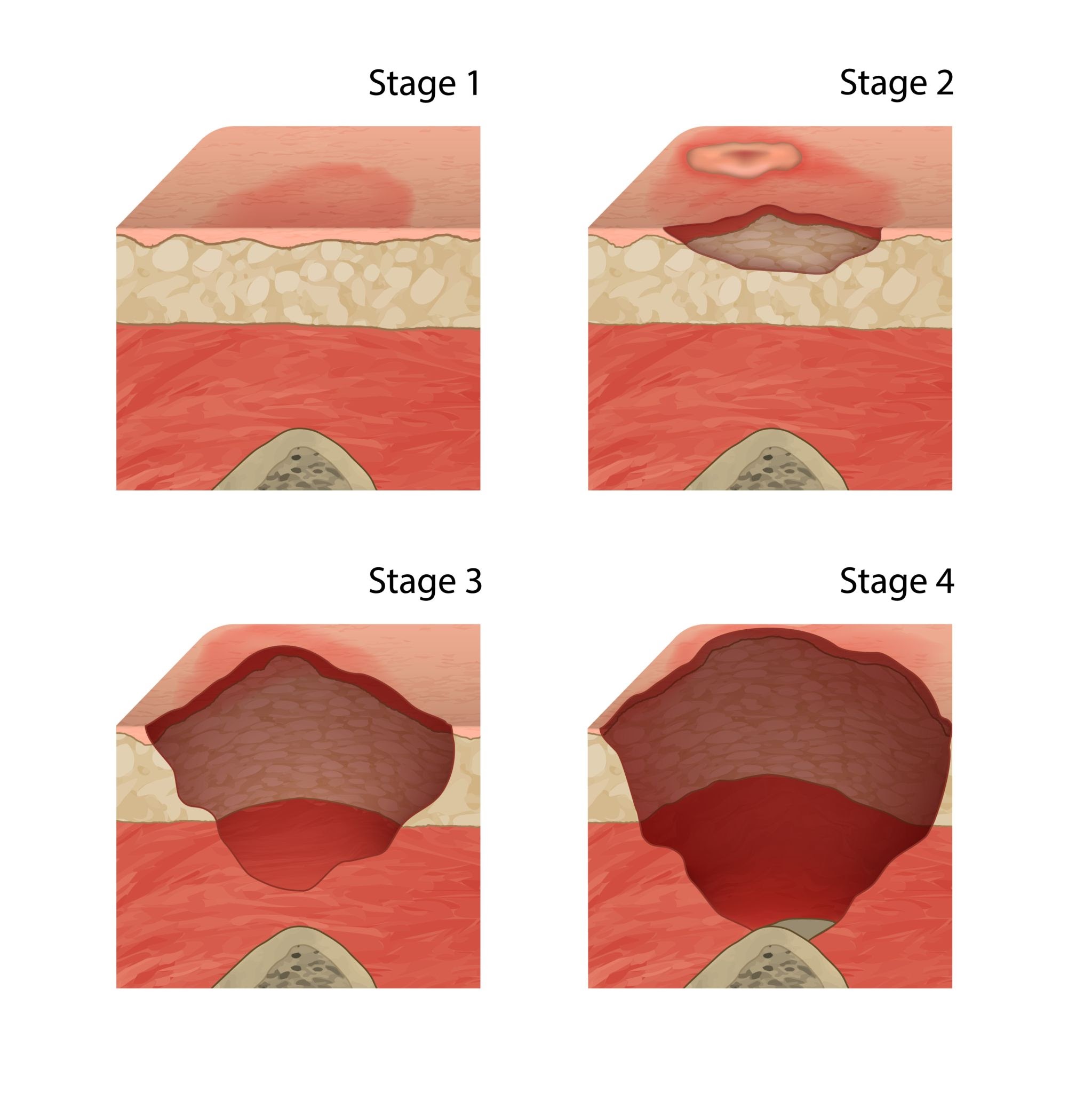
Choice D reason: A stage 2 pressure injury involves partial-thickness loss of the dermis. It typically presents as a shallow, open ulcer with a red-pink wound bed without slough. It may also present as an intact or open/ruptured serum-filled blister. This stage specifically involves the epidermis and the uppermost layers of the dermis, representing a significant break in the skin's protective barrier.
Correct Answer is B
Explanation
Choice A reason: The tympanic route involves placing a probe into the external ear canal. While fast and generally well-tolerated, it requires direct physical contact with a sensitive sensory organ and correct positioning of the earlobe to straighten the canal. It is considered more invasive than the axillary route because it enters a body cavity.
Choice B reason: The axillary route is considered the least invasive as the thermometer is placed in the skin fold of the armpit, requiring no entry into any body orifice or mucous membrane contact. It is often the preferred method for initial screenings or for patients who cannot tolerate other methods, although it is generally less accurate than core or oral temperatures.
Choice C reason: The oral route requires the patient to hold a probe under the tongue in the sublingual pocket. While common, it is more invasive than the axillary method because it involves a mucous membrane and requires patient cooperation to avoid biting the probe. It can also be influenced by recent intake of hot or cold liquids.
Choice D reason: The rectal route is the most invasive method for temperature measurement, as it requires the insertion of a lubricated probe into the anal canal. While it provides the most accurate reflection of core body temperature, it carries the highest risk of injury, discomfort, and psychological distress for the patient.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today