A nurse is documenting a stage 4 pressure injury. Which of the following descriptions accurately fits this stage?
Full-thickness tissue loss extending to bone or tendon.
Intact skin with nonblanchable erythema.
Full-thickness skin loss with visible fat.
Partial-thickness skin loss involving the dermis and epidermis.
The Correct Answer is A
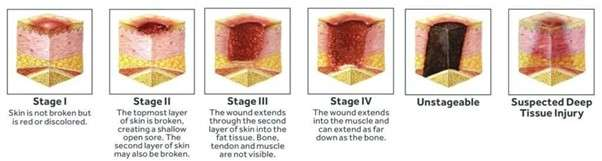
A. Full-thickness tissue loss extending to bone or tendon: A Stage 4 pressure injury is characterized by full-thickness tissue loss where fascia, muscle, tendon, ligament, cartilage, or bone are directly exposed or directly palpable. Undermining and tunneling are often extensive at this stage.
B. Intact skin with nonblanchable erythema: This describes a Stage 1 pressure injury.
C. Full-thickness skin loss with visible fat: This describes a Stage 3 pressure injury, which extends through the dermis and involves the subcutaneous fat but does not expose bone, tendon, or muscle.
D. Partial-thickness skin loss involving the dermis and epidermis: This describes a Stage 2 pressure injury, which involves only the partial loss of skin layers.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. Presence of slough or eschar: Both Stage 2 and Stage 3 injuries may eventually develop some slough if they deteriorate or if they are mismanaged. However, slough and eschar are defining characteristics of an unstageable injury if they obscure the wound base. A clean Stage 2 injury will not have slough or eschar.
B. Nonblanchable erythema: Nonblanchable erythema is the defining characteristic of a Stage 1 pressure injury, which involves intact skin. Stage 2 and Stage 3 both involve skin loss.
C. Exposed muscle or bone: Exposed muscle or bone indicates a Stage 4 pressure injury.
D. Partial-thickness skin loss: A Stage 2 pressure injury is defined by partial-thickness loss of the dermis. A Stage 3 pressure injury is defined by full-thickness tissue loss involving the subcutaneous fat. This difference in thickness is the key distinction.
Correct Answer is C
Explanation
A. Normal healing process: Normal healing involves serous or serosanguineous drainage. Purulent drainage signifies a complication (infection).
B. Eschar formation: Eschar is hard, black, necrotic tissue; it is not a type of drainage.
C. Presence of infection: Purulent drainage (pus)-which is thick, opaque, and often yellow, green, or brown-is composed of dead white blood cells, bacteria, and tissue debris, indicating a localized bacterial infection.
D. Granulation tissue: Granulation tissue is bright red, moist, and bumpy tissue, which is a sign of the proliferative phase of normal healing, not the fluid component.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today