A patient with darker skin tones is suspected of having a stage 1 pressure ulcer. Which clinical assessment finding would most support this diagnosis?
Presence of a blister on the skin.
Exposed bone or muscle.
A localized area of skin that is warm to the touch.
Presence of a deep crater in the skin.
The Correct Answer is C
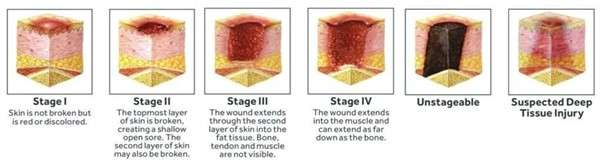
A. Presence of a blister on the skin: A blister, usually indicating separation of the epidermis and dermis, is characteristic of a Stage 2 pressure injury or a Deep Tissue Pressure Injury (DTPI).
B. Exposed bone or muscle: Exposed bone or muscle signifies a Stage 4 pressure injury, which is full-thickness skin and tissue loss.
C. A localized area of skin that is warm to the touch: In darker skin tones, a Stage 1 pressure injury (which is intact skin) is often identified by changes in skin temperature (localized warmth or coolness) or consistency (edema, firmness, or boggy feel), rather than visible reddening. The area may appear darker, taut, or purplish, and the warmth is due to the underlying inflammatory response.
D. Presence of a deep crater in the skin: A deep crater suggests a significant loss of tissue depth, characteristic of a Stage 3 or 4 pressure injury.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. The patient has a high-protein diet: A high-protein diet promotes healing, which would decrease the risk of wound separation.
B. Patient is ambulating frequently post-surgery: Frequent, gentle ambulation improves circulation and general strength, which helps recovery and reduces complications like infection and DVT.
C. The patient has a history of chronic coughing and sneezing: This is the most strongly contributing factor. Any activity that suddenly and dramatically increases intra-abdominal pressure (like severe coughing, vomiting, straining, or sneezing) can place extreme tension on a healing surgical incision, leading to separation (dehiscence) and potentially organ protrusion (evisceration).
D. Patient is on immunosuppressant therapy: This is a factor that impairs healing and increases infection risk, but it does not directly cause the mechanical failure of the incision, which is the immediate cause of evisceration.
Correct Answer is C
Explanation
A. Full-thickness skin loss with visible fat.: This describes a Stage 3 pressure injury.
B. Partial-thickness skin loss involving the epidermis and dermis.: This describes a Stage 2 pressure injury.
C. Intact skin with nonblanchable erythema.: A Stage 1 pressure injury is characterized by localized intact skin with a persistent area of redness (erythema) that does not blanch (turn white) when light pressure is applied. This nonblanching indicates deep tissue damage caused by pressure.
D. Deep injury extending down to the bone.: This describes a Stage 4 pressure injury.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today