A nurse is reinforcing teaching with a client who reports constipation. Which of the following should the nurse discuss as causes of constipation? (Select all that apply.)
Ignoring the urge to defecate
Increased fiber in the diet
Excessive laxative use
Increased activity
Correct Answer : A,C
Choice A reason: Ignoring the urge to defecate is a cause of constipation, as it can lead to hardening and accumulation of stool in the colon. The nurse should advise the client to respond to the urge to defecate as soon as possible and to establish a regular bowel routine.
Choice B reason: Increased fiber in the diet is not a cause of constipation, but rather a prevention measure. Fiber helps to soften the stool and increase its bulk, which facilitates its passage through the colon. The nurse should encourage the client to consume adequate amounts of fiber from fruits, vegetables, whole grains, and legumes.
Choice C reason: Excessive laxative use is a cause of constipation, as it can interfere with the normal functioning of the colon and cause dependency. The nurse should instruct the client to avoid using laxatives unless prescribed by the provider and to use them only for a short period of time.
Choice D reason: Increased activity is not a cause of constipation, but rather a prevention measure. Activity helps to stimulate the peristalsis of the colon and promote bowel movements. The nurse should recommend the client to engage in moderate physical activity for at least 30 minutes a day
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Respiratory rate 28/min is not a sign of effective oxygen therapy, as it indicates tachypnea, which is a rapid breathing rate. Tachypnea can be caused by hypoxia, anxiety, fever, or pain.
Choice B reason: Pink mucous membranes are a sign of effective oxygen therapy, as they indicate adequate oxygenation of the tissues. Pink mucous membranes are a normal finding, while pale, cyanotic, or jaundiced mucous membranes can indicate hypoxia or other problems.
Choice C reason: Heart rate 110/min is not a sign of effective oxygen therapy, as it indicates tachycardia, which is a rapid heart rate. Tachycardia can be caused by hypoxia, stress, dehydration, or infection.
Choice D reason: Restlessness is not a sign of effective oxygen therapy, as it indicates agitation, anxiety, or discomfort. Restlessness can be caused by hypoxia, pain, or medication side effects.
Correct Answer is D
Explanation
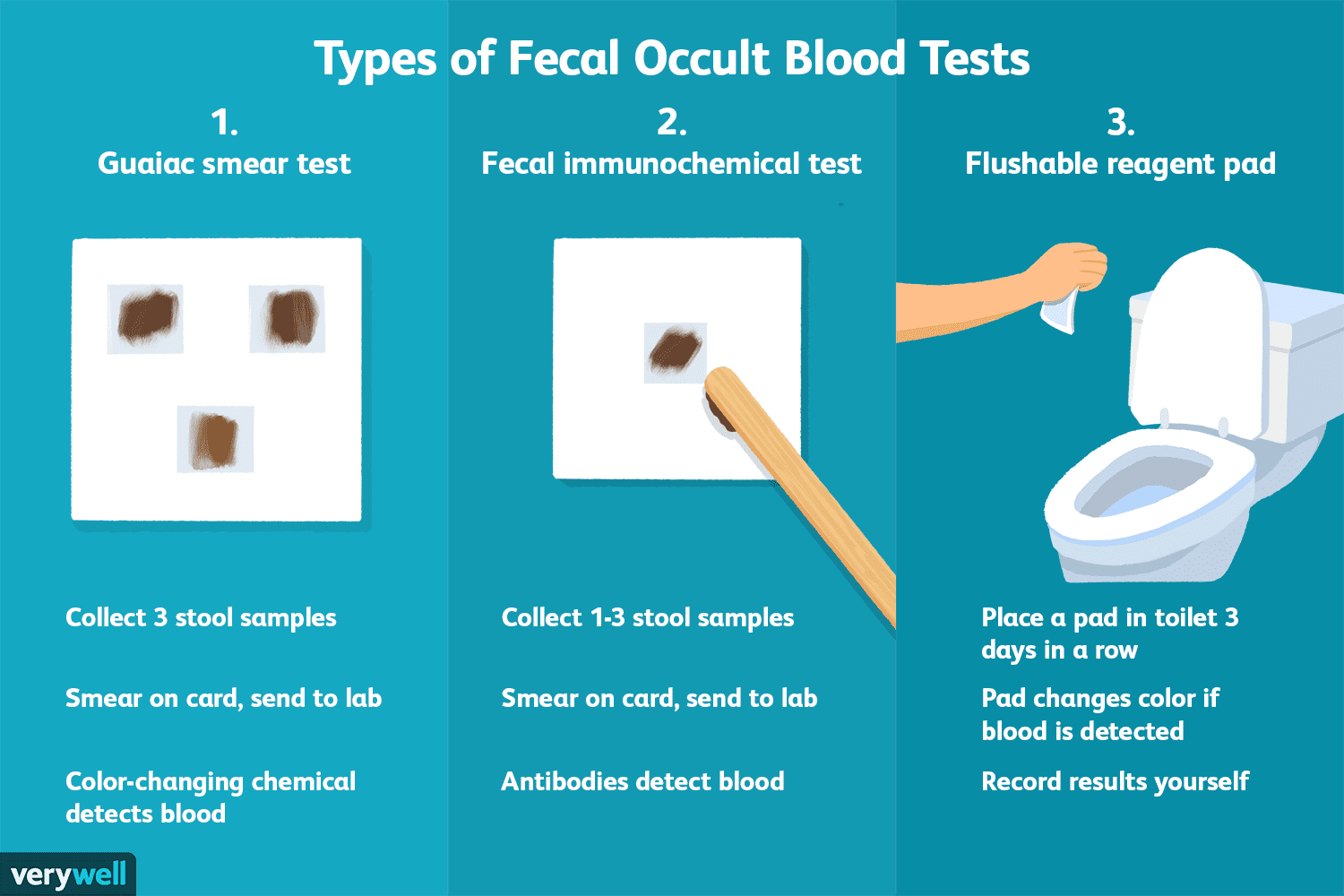
Choice A reason: Bacteria are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Bacteria are microorganisms that do not contain hemoglobin.
Choice B reason: Fat is not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Fat is a lipid that does not contain hemoglobin.
Choice C reason: Parasites are not detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Parasites are organisms that live in or on another host and do not contain hemoglobin.
Choice D reason: Blood is detected by the stool guaiac test. The stool guaiac test is a chemical test that reacts with hemoglobin, a protein found in red blood cells. Blood can indicate bleeding in the gastrointestinal tract, which can be caused by various conditions such as ulcers, polyps, or cancer.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today