A nurse is teaching a group of newly licensed nurses about the Braden scale. Which of the following responses by a newly licensed nurse indicates an understanding of the teaching?
"The client's age is part of the measurement."
"Each element has a range from one to five points."
"The higher the score, the higher the pressure injury risk."
"The scale measures six elements."
The Correct Answer is D
Choice A Reason:
"The client's age is part of the measurement." - This is not accurate. The Braden scale does not include the client's age as part of the assessment. The elements evaluated are related to factors such as sensory perception, mobility, and nutrition, not age.
Choice B Reason:
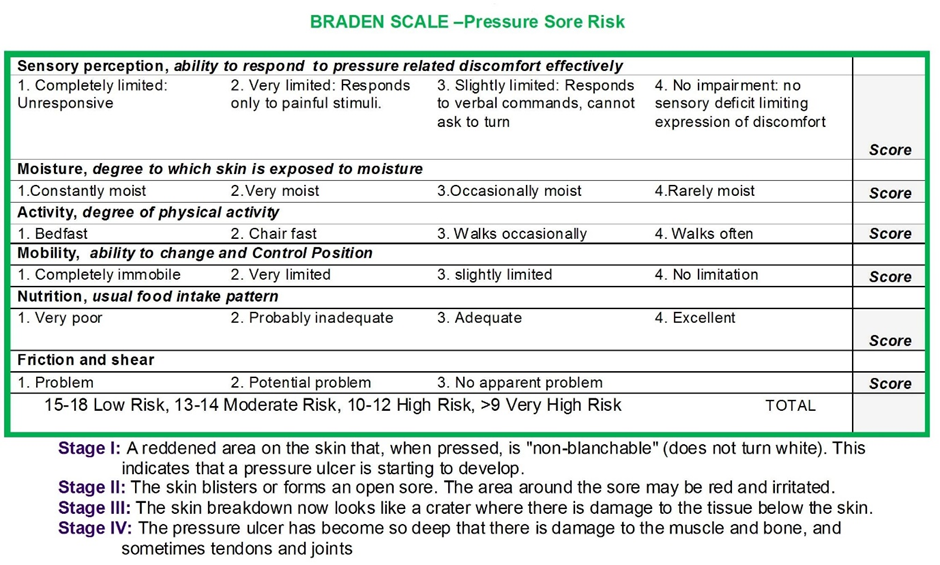
"Each element has a range from one to five points." The Braden scale assesses a client's risk for developing pressure ulcers by evaluating six different elements: sensory perception, moisture, activity, mobility, nutrition, and friction/shear. Each of these elements is scored from 1 to 5 points, with a higher score indicating better functioning or less risk for developing pressure injuries. Understanding that each element is scored on a scale from 1 to 5 is a fundamental aspect of using the Braden scale effectively.
Choice C Reason:
"The higher the score, the higher the pressure injury risk." - This is incorrect. In the Braden scale, a higher score indicates a lower risk of developing pressure injuries. Higher scores mean that the client has better functioning in the assessed elements, which reduces their risk.
Choice D Reason:
"The scale measures six elements." - This statement is true. The Braden scale measures six elements: sensory perception, moisture, activity, mobility, nutrition, and friction/shear. However, the response does not demonstrate an understanding of how each element is scored, which is the main focus of the scale.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason:
Percussion is useful for assessing the presence of gas, fluid, or solid masses in the abdomen. Resonance might indicate normal air-filled intestines, while dullness could suggest fluid or mass. However, percussion is not the first action in an acute setting of sudden severe pain because it does not provide immediate information that could be life-saving. It is a later step in the physical examination.
Choice B Reason:
Using the diaphragm of a stethoscope to listen for bowel sounds: Absence of bowel sounds might suggest a paralytic ileus, while hyperactive sounds could indicate a bowel obstruction. However, in the context of sudden, severe abdominal pain postoperatively, auscultation is not the first priority.
Choice C Reason:
Visual inspection is the first step because it can quickly reveal critical signs such as swelling, distention, redness, or evidence of wound complications like dehiscence or evisceration. Identifying these signs early allows for rapid intervention, which could be life-saving. This is why exposing and inspecting the abdomen is the priority in the context of sudden severe pain following surgery.
Choice D Reason:
Palpation can help assess for tenderness, rigidity, or masses in the abdomen, which might indicate infection, bleeding, or other complications. However, palpation could potentially worsen a condition such as an evisceration or dehiscence, or cause additional pain. Therefore, palpation should be done only after the visual inspection and with great caution in the presence of severe pain.
Correct Answer is B
Explanation
Choice A Reason:
"The surgeon will only place the colostomy if it is necessary." While this provides information, it may not fully address the client's emotional concerns and does not encourage open communication.
Choice B Reason:
"You are worried about having to wear a colostomy bag?" This response acknowledges the client's feelings and opens the door for further discussion about their concerns. It allows the nurse to address the client's worries, provide information, and offer emotional support.
Choice C Reason:
"Let's wait until after the surgery to discuss your concerns about your colostomy." Delaying the discussion may increase the client's anxiety and make them feel unheard.
Choice D Reason:
"Have you ever known someone who has a colostomy?" While this question may be relevant, it doesn't directly address the client's current feelings or concerns. It's important to acknowledge and validate the client's emotions before exploring their experiences or providing information.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today