A nurse notices bright red sanguineous drainage on a surgical dressing shortly after surgery. What is the most appropriate initial action?
Administer prophylactic antibiotics as prescribed.
Apply a pressure dressing and notify the provider immediately.
Elevate the affected area above the level of the heart to reduce blood flow.
Clean the wound and replace the dressing with a new sterile dressing.
The Correct Answer is B
A. Administer prophylactic antibiotics as prescribed: Antibiotics address infection, not acute bleeding.
B. Apply a pressure dressing and notify the provider immediately: This is the most appropriate initial action. Since the drainage is bright red (active bleeding) and occurred shortly after surgery, the nurse must immediately attempt to control the bleeding by applying firm, direct pressure (pressure dressing) over the site. Simultaneously, the surgeon or healthcare provider must be notified immediately as this finding may indicate a failed suture line or internal hemorrhage requiring urgent intervention.
C. Elevate the affected area above the level of the heart to reduce blood flow: This is appropriate for extremity bleeding, but for an abdominal or thoracic surgical site, this maneuver is ineffective or contraindicated. Direct pressure is necessary.
D. Clean the wound and replace the dressing with a new sterile dressing: Removing the original dressing can disrupt clot formation and lead to further blood loss. The priority is to stop the bleeding, not to clean or replace the dressing. If the dressing is soaked, the nurse should reinforce the dressing while applying pressure.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. A patient with adequate hydration and skin care regimen.Adequate hydration and a good skin care regimen are preventive measures that significantly decrease the risk of developing a pressure injury.
B. An immobile patient with poor nutritional status.Immobility (prolonged, unrelieved pressure and shear) is the primary mechanical cause of pressure injuries. Poor nutritional status (specifically, low protein and poor hydration) compromises the integrity of the skin and the body's ability to repair tissue, drastically multiplying the overall risk.
C. A mobile patient with a history of diabetes.While diabetes is a risk factor due to poor circulation and neuropathy, a mobile patient can independently relieve pressure, which is the most critical factor in prevention. Therefore, they are at a lower risk than an immobile patient.
D. A patient who regularly changes position every hour.Regular repositioning (typically every two hours in bed, or more frequently in a chair) is the single most effective intervention for preventing pressure injuries. This patient is actively mitigating their risk.
Correct Answer is C
Explanation
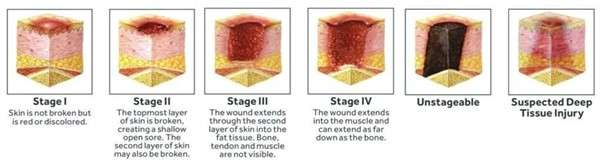
A. Full-thickness skin loss with visible fat.: This describes a Stage 3 pressure injury.
B. Partial-thickness skin loss involving the epidermis and dermis.: This describes a Stage 2 pressure injury.
C. Intact skin with nonblanchable erythema.: A Stage 1 pressure injury is characterized by localized intact skin with a persistent area of redness (erythema) that does not blanch (turn white) when light pressure is applied. This nonblanching indicates deep tissue damage caused by pressure.
D. Deep injury extending down to the bone.: This describes a Stage 4 pressure injury.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today