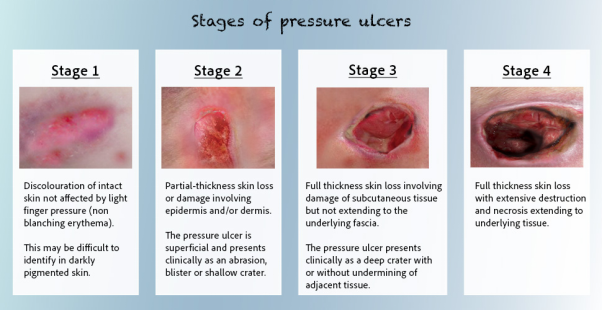
A patient has a pressure injury on their sacrum characterized by partial-thickness skin loss with exposed dermis, pink wound bed, and no slough or eschar. What stage of pressure injury does this indicate?
Stage 2
Stage 1
Unstageable
Stage 3
The Correct Answer is A
A. Stage 2: The definition of a Stage 2 pressure injury is partial-thickness skin loss with exposed dermis. The wound bed is viable, pink or red, moist, and may present as an intact or ruptured serum-filled blister. Critically, there is no granulation tissue, slough, or eschar.
B. Stage 1: A Stage 1 injury involves intact skin (no skin loss).
C. Unstageable: An Unstageable injury is one where the full depth cannot be determined due to obscuring slough or eschar, which are explicitly absent in this description.
D. Stage 3: A Stage 3 injury involves full-thickness skin loss with visible adipose (fat) tissue.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
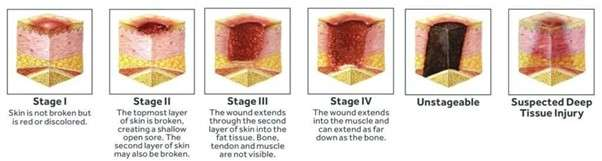
A. Full-thickness tissue loss extending to bone or tendon: A Stage 4 pressure injury is characterized by full-thickness tissue loss where fascia, muscle, tendon, ligament, cartilage, or bone are directly exposed or directly palpable. Undermining and tunneling are often extensive at this stage.
B. Intact skin with nonblanchable erythema: This describes a Stage 1 pressure injury.
C. Full-thickness skin loss with visible fat: This describes a Stage 3 pressure injury, which extends through the dermis and involves the subcutaneous fat but does not expose bone, tendon, or muscle.
D. Partial-thickness skin loss involving the dermis and epidermis: This describes a Stage 2 pressure injury, which involves only the partial loss of skin layers.
Correct Answer is B
Explanation
A. Administer prophylactic antibiotics as prescribed: Antibiotics address infection, not acute bleeding.
B. Apply a pressure dressing and notify the provider immediately: This is the most appropriate initial action. Since the drainage is bright red (active bleeding) and occurred shortly after surgery, the nurse must immediately attempt to control the bleeding by applying firm, direct pressure (pressure dressing) over the site. Simultaneously, the surgeon or healthcare provider must be notified immediately as this finding may indicate a failed suture line or internal hemorrhage requiring urgent intervention.
C. Elevate the affected area above the level of the heart to reduce blood flow: This is appropriate for extremity bleeding, but for an abdominal or thoracic surgical site, this maneuver is ineffective or contraindicated. Direct pressure is necessary.
D. Clean the wound and replace the dressing with a new sterile dressing: Removing the original dressing can disrupt clot formation and lead to further blood loss. The priority is to stop the bleeding, not to clean or replace the dressing. If the dressing is soaked, the nurse should reinforce the dressing while applying pressure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today