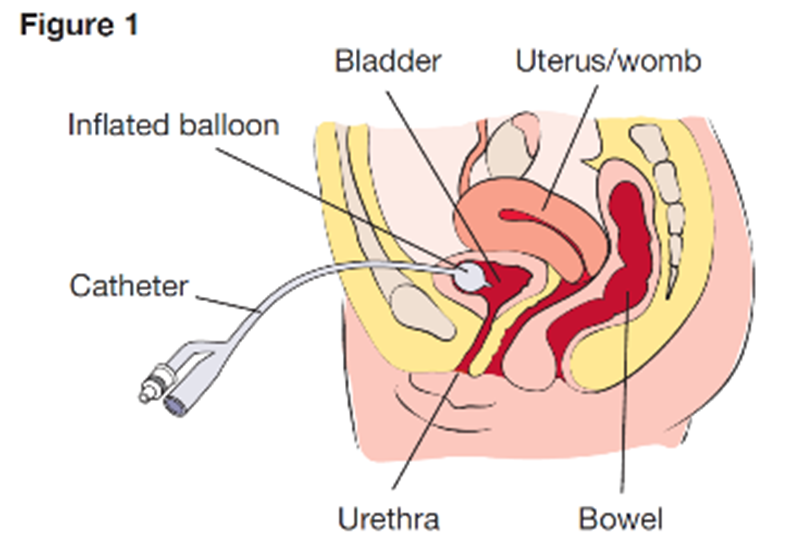
Which assessment should the home health nurse include during a routine home visit for a client who was discharged home with a suprapubic catheter?
Observe insertion site.
Palpate flank area.
Measure abdominal girth.
Assess perineal area.
The Correct Answer is A
Choice A reason: Observing the insertion site of the suprapubic catheter is an essential assessment for the home health nurse, as this can help detect any signs of infection, inflammation, or leakage. Therefore, this is the correct choice.
Choice B reason: Palpating the flank area is not a necessary assessment for the home health nurse, as this is not related to the suprapubic catheter. This is a distractor choice.
Choice C reason: Measuring abdominal girth is not a relevant assessment for the home health nurse, as this is not affected by the suprapubic catheter. This is another distractor choice.
Choice D reason: Assessing the perineal area is not an important assessment for the home health nurse, as this is not involved in the suprapubic catheter. This is another distractor choice.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","D","E"]
Explanation
Choice A reason: Providing diet low in phosphorus is not a relevant intervention for a client with cirrhosis of the liver. Phosphorus is a mineral that helps maintain bone health and acid-base balance. Cirrhosis of the liver does not affect phosphorus levels, but it can cause low calcium levels due to impaired vitamin D metabolism. The nurse should provide a diet high in calcium and vitamin D to prevent osteoporosis and fractures.
Choice B reason: This is a correct answer because noting signs of swelling and edema is an important intervention for a client with cirrhosis of the liver. Cirrhosis of the liver is a chronic condition that causes scarring and damage to the liver tissue, impairing its function and blood flow. This can lead to portal hypertension, which is increased pressure in the portal vein that carries blood from the digestive organs to the liver. Portal hypertension can cause fluid accumulation in the abdomen (ascites) and legs (peripheral edema). The nurse should assess the client's weight, fluid intake and output, abdominal girth, and extremity circumference.
Choice C reason: Increasing oral fluid intake to 1,500 mL daily is not a suitable intervention for a client with cirrhosis of the liver. Fluid intake should be individualized based on the client's fluid status, electrolyte levels, and urine output. Increasing fluid intake may worsen fluid retention and electrolyte imbalance in clients with cirrhosis of the liver. The nurse should restrict fluid intake to 1,000 to 1,500 mL daily or as prescribed by the healthcare provider.
Choice D reason: This is a correct answer because monitoring abdominal girth is an essential intervention for a client with cirrhosis of the liver. Abdominal girth is a measurement of the circumference of the abdomen at the level of the umbilicus. It reflects the amount of fluid in the peritoneal cavity, which can increase due to portal hypertension and hypoalbuminemia in clients with cirrhosis of the liver. The nurse should measure and record abdominal girth daily or more frequently as indicated.
Choice E reason: This is a correct answer because reporting serum albumin and globulin levels is a significant intervention for a client with cirrhosis of the liver. Albumin and globulin are types of proteins that are synthesized by the liver and have various functions in the body, such as maintaining fluid balance, transporting hormones and drugs, and fighting infections. Cirrhosis of the liver can cause low albumin levels due to reduced synthesis and increased loss through ascites or urine. Low albumin levels can cause edema, malnutrition, and increased risk of infection. Cirrhosis of the liver can also cause high globulin levels due to chronic inflammation or immune response. High globulin levels can indicate autoimmune diseases, infections, or malignancies. The nurse should monitor and report serum albumin and globulin levels as they reflect liver function and overall health status.
Correct Answer is A
Explanation
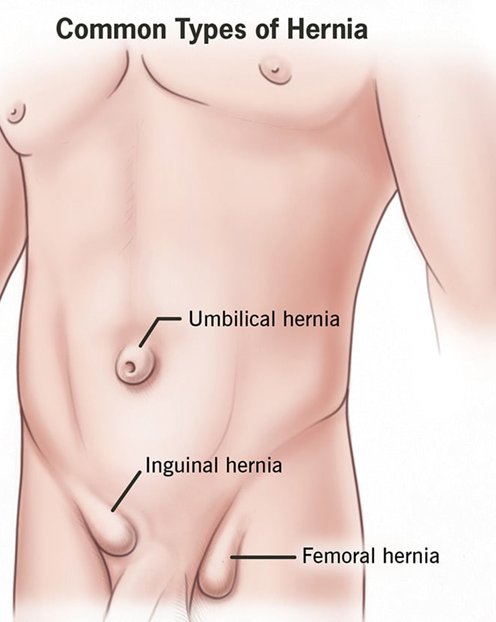
Choice A reason: This hernia is a normal variation that resolves without treatment is a correct explanation for the nurse to provide, as this refers to an umbilical hernia, which is a common and harmless condition in infants that usually disappears by age 2. Therefore, this is the correct choice.
Choice B reason: An abdominal binder can be worn daily to reduce the protrusion is not an appropriate explanation for the nurse to provide, as this is not an effective or recommended method to treat a hernia. This is a distractor choice.
Choice C reason: Restrictive clothing will be adequate to help the hernia go away is not a relevant explanation for the nurse to provide, as this does not affect the hernia or its resolution. This is another distractor choice.
Choice D reason: The quarter should be secured with an elastic bandage wrap is not a sensible explanation for the nurse to provide, as this is a folk remedy that has no scientific basis and can cause skin irritation and infection. This is another distractor choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today