The nurse is assessing the abdomen of the client with an undiagnosed disorder. In which sequence would the nurse conduct the abdominal assessment? (Use all options.)
Palpation.
Inspection.
Auscultation.
Percussion.
The Correct Answer is B
Inspection, followed by Auscultation, Percussion, and Palpation. Inspection assesses for abdominal contour, symmetry, any visible masses, scars or other abnormalities. Auscultation assesses bowel sounds, and Percussion assesses for any areas of tenderness, and to determine the presence of fluid, gas or masses. Palpation assesses for any masses, areas of tenderness, organ size or other abnormalities. This is the order that allows the nurse to assess the abdomen systematically and accurately.
A: Palpation comes last because it can stimulate bowel sounds, which can make the nurse miss some of the sounds while auscultating.
C: Auscultation must be done before percussion and palpation to prevent altering bowel sounds.
D: Percussion comes before palpation to avoid altering the underlying structures of the abdomen.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
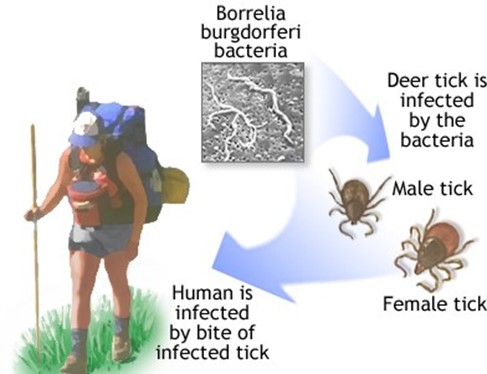
36 to 48 hours. Lyme disease is caused by the bacterium Borrelia burgdorferi, which is transmitted to humans through the bite of infected black-legged ticks. The tick must be attached to the skin for at least 36 to 48 hours for the bacterium to be transmitted. The nurse should advise the client to seek medical attention promptly.
Choice B is incorrect because the tick must be attached for a longer duration of time for the bacterium to be transmitted.
Choice C is incorrect because the tick must be attached for a longer duration of time for the bacterium to be transmitted.
Choice D is incorrect because the tick must be attached for a longer duration of time for the bacterium to be transmitted.
Correct Answer is B
Explanation
Choice A is incorrect because stuporous is a state of reduced consciousness, and does not describe the posturing observed in the client.
Choice B is correct because decerebrate posturing is characterized by extension of the arms, wrists, and fingers, and extension and internal rotation of the legs, with plantar flexion of the feet.
Choice C is incorrect - Decorticate posturing is characterized by flexion of the arms, wrists, and fingers, extension, internal rotation, and adduction of the legs, with plantar flexion of the feet. This is caused by damage to the cerebral cortex and is indicative of a neurological problem.
Choice D is incorrect because flaccidity is a state of complete lack of muscle tone, and does not describe the posturing observed in the client.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today