The nurse notes that a newborn's white blood cell count (WBC) is 15,000. The nurse is aware that:.
This indicates a severe infection.
This is a normal WBC for a newborn.
This is a lab error.
You must call the doctor.
The Correct Answer is B
Choice A rationale:
A white blood cell count of 15,000 does not necessarily indicate a severe infection. In newborns, WBC counts are typically higher than in adults, and they gradually decrease over the first few days after birth. A value of 15,000 falls within the normal range for a newborn and is not indicative of a severe infection.
Choice B rationale:
A white blood cell count of 15,000 is considered a normal range for a newborn. Newborns have higher WBC counts as a natural response to the stress of birth and exposure to the outside environment. The immune system is still developing, and elevated WBC counts are normal during this period.
Choice C rationale:
Assuming there are no other indications of lab error, such as abnormal results in other tests, it would be premature to label the WBC count as a lab error. Additionally, healthcare professionals should always consider the overall clinical picture before assuming a lab error based on a single result.
Choice D rationale:
There is no immediate need to call the doctor based solely on the WBC count of 15,000. Medical decisions should be made in the context of the newborn's overall clinical condition, and a single lab result does not warrant an immediate call to the doctor.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","C","D","E"]
Explanation
Choice A rationale:
Drying the baby thoroughly is not directly related to assessing the successful transition of the respiratory system. It is essential for warmth and comfort but does not provide specific information about the respiratory system.
Choice B rationale:
Suctioning the mouth and nose with a bulb syringe to clear mucus is important to ensure the airways are clear and the newborn can breathe effectively. This action helps assess the airway patency and successful initiation of breathing.
Choice C rationale:
Observing the chest and abdomen is crucial to assess the respiratory effort and symmetry. Normal chest movements and equal rise and fall of the abdomen indicate a successful transition of the respiratory system.
Choice D rationale:
Counting the number of respirations per minute is essential to determine if the respiratory rate falls within the expected reference range (around 30-60 breaths per minute for a newborn) and if there are any irregularities.
Choice E rationale:
Observing the color of the mucous membranes is important as cyanosis (blue discoloration) may indicate inadequate oxygenation. Pink mucous membranes are a positive sign, indicating a successful transition of the respiratory system.
Correct Answer is ["A","C","D","F"]
Explanation
Choice A rationale:
The newborn reflex called "rooting”. is characterized by turning the head and opening the mouth when the cheek or mouth area is touched. This reflex helps the newborn find the mother's breast for feeding.
Choice B rationale:
"Stepping”. is a newborn reflex where they make stepping movements when held upright with their feet touching a solid surface. This reflex is present at birth but tends to disappear after a few weeks.
Choice C rationale:
The "Moro”. reflex is also known as the startle reflex. It is elicited by a sudden loss of support or loud noise, causing the newborn to throw their arms and legs out and then bring them back in. This reflex usually disappears around 3 to 4 months of age.
Choice D rationale:
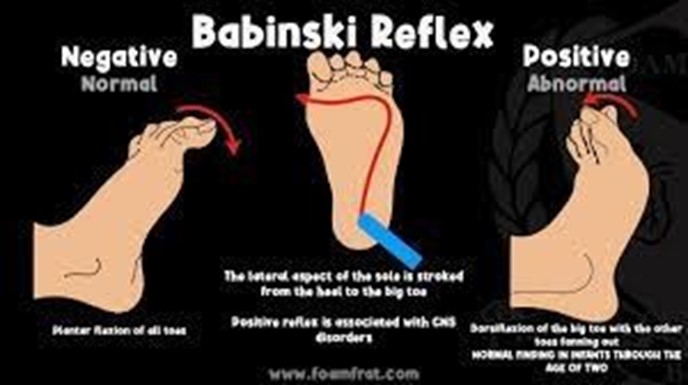
The "Babinski”. reflex is characterized by the extension of the big toe and fanning of the other toes when the sole of the foot is stroked. This reflex is present in newborns and should disappear by around 12 months of age.
Choice E rationale:
"Running”. is not a recognized newborn reflex. There is no reflex with this name related to newborns.
Choice F rationale:
The "gag”. reflex is present in newborns and helps protect the airway by causing a gagging response when the back of the throat is stimulated.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today