The nurse observes that there are reddened areas on the cheekbones of a client receiving oxygen per nasal cannula at 3 L/minute, and the client's oxygen saturation level is 92%. Which intervention would the nurse implement?
Decrease the flow rate to 1 L/minute.
Place padding around the cannula tubing.
Apply lubricant to the cannula tubing.
Discontinue the use of the nasal cannula.
The Correct Answer is B
Choice A Reason: This is incorrect because decreasing the flow rate to 1 L/minute can compromise the client's oxygenation and worsen hypoxia. The client's oxygen saturation level is below the normal range of 95% to 100%.
Choice B Reason: This is correct because placing padding around the cannula tubing can prevent pressure ulcers and skin breakdown caused by friction and irritation from the tubing.
Choice C Reason: This is incorrect because applying lubricant to the cannula tubing can increase the risk of infection and inflammation of the nasal mucosa. Lubricant should be applied sparingly to the nares only if needed.
Choice D Reason: This is incorrect because discontinuing the use of the nasal cannula can endanger the client's life and cause respiratory failure. The client needs supplemental oxygen to maintain adequate oxygenation.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This is incorrect because palpating the suprapubic region for distention can be inaccurate and unreliable, as it can be affected by factors such as obesity, abdominal muscle tone, and bowel gas.
Choice B Reason: This is correct because scanning the client's bladder after voiding can measure the post-void residual urine volume, which indicates the amount of urine left in the bladder after urination. A high post-void residual urine volume can indicate urinary retention.
Choice C Reason: This is incorrect because reviewing the chart for number of voids over last 24 hours can provide information about the frequency of urination, but not the amount or completeness of urination.
Choice D Reason: This is incorrect because evaluating the client for urinary incontinence can assess the involuntary loss of urine, but not the ability to empty the bladder completely.
Correct Answer is A
Explanation
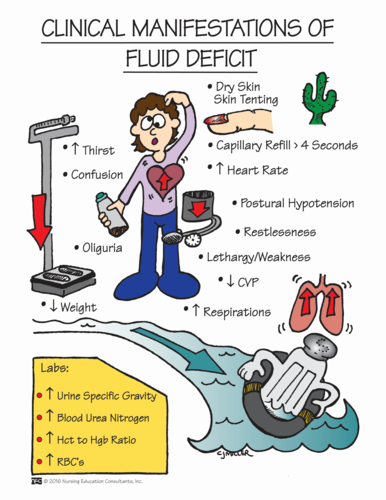
Choice A Reason: This is correct because fluid volume deficit is a life-threatening condition that can result from diarrhea and fecal incontinence. The nurse should monitor the client's fluid intake and output, electrolytes, weight, urine specific gravity, and skin turgor.
Choice B Reason: This is incorrect because bowel incontinence is a significant problem that can affect the client's dignity, comfort, and skin integrity, but it is not as urgent as fluid volume deficit. The nurse should implement a bowel management program and provide appropriate hygiene and skin care.
Choice C Reason: This is incorrect because caregiver role strain is a potential problem that can affect the parent's well-being and ability to provide care, but it is not as critical as fluid volume deficit. The nurse should assess the parent's coping skills, support system, and respite needs.
Choice D Reason: This is incorrect because impaired bed mobility is a chronic problem that can affect the client's functional status and quality of life, but it is not as serious as fluid volume deficit. The nurse should assist the client with positioning, turning, transferring, and exercising.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today