Which three of the following are common adverse effects of beta-blockers?
Bronchospasm
Bradycardia
Hyperglycemia
Fatigue
Correct Answer : A,B,D
A. Bronchospasm: Non-selective beta-blockers inhibit beta-2 receptors located in the bronchial smooth muscle, leading to unintended constriction of the airways. This physiological response significantly increases airway resistance and can trigger acute respiratory distress in patients with underlying asthma or COPD. Clinicians must exercise extreme caution when prescribing these agents to individuals with reactive airway diseases.
B. Bradycardia: Beta-adrenoceptor antagonists decrease the firing rate of the sinoatrial node and slow conduction through the atrioventricular node. This negative chronotropic effect results in a reduced heart rate, which is a primary pharmacological action of the drug class. Excessive blockade can lead to symptomatic bradycardia, requiring a dose adjustment or discontinuation to maintain adequate cardiac output.
C. Hyperglycemia: Beta-blockers do not typically cause an elevation in blood glucose levels as a primary adverse effect. Instead, they are known to mask the sympathetic symptoms of hypoglycemia, such as tachycardia and tremors, which can be dangerous for diabetic patients. They may also slightly impair insulin release, but they are not categorized as hyper-glycemic agents.
D. Fatigue: The reduction in cardiac output and the blockade of peripheral beta-receptors often lead to a profound sense of lethargy or exercise intolerance. Patients frequently report feeling tired because the heart cannot increase its rate sufficiently to meet increased metabolic demands during physical activity. This is one of the most common reasons for patient non-compliance with beta-blocker therapy.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
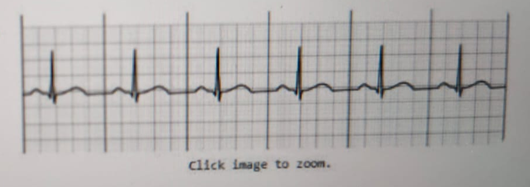
A. Ventricular Tachycardia: This rhythm would be characterized by a rapid rate and wide, bizarre QRS complexes without visible P waves. The provided strip shows narrow QRS complexes and a regular rhythm, which is inconsistent with ventricular tachycardia. This patient is not demonstrating a life-threatening ventricular arrhythmia.
B. Normal Sinus Rhythm: The strip displays a regular rhythm with a P wave preceding every QRS complex, followed by a T wave. The rate is approximately 60 to 70 beats per minute, and the complexes are narrow and uniform. This represents the standard, healthy electrical conduction of the heart starting from the sinoatrial node.
C. Ventricular Fibrillation: Ventricular fibrillation would appear as a chaotic, wavy baseline with no identifiable QRS complexes or P waves. The strip clearly shows organized electrical activity and distinct mechanical contractions. This rhythm is incompatible with the stable, organized complexes seen in the client's telemetry.
D. Atrial Fibrillation: Atrial fibrillation is marked by an irregularly irregular rhythm and the absence of distinct P waves. The telemetry strip provided shows a very regular R-R interval and clear, consistent P waves before each contraction. Therefore, it does not meet the criteria for a diagnosis of atrial fibrillation.
Correct Answer is D
Explanation
A. Discourage walking in order to limit pain: Physical inactivity promotes further vascular stasis and muscle atrophy in the lower extremities. While claudication causes discomfort, complete avoidance of movement prevents the development of collateral circulation. Reduced mobility exacerbates the underlying pathology of arterial insufficiency and impairs long-term functional outcomes.
B. Encourage extended periods of sitting or standing: Prolonged static positioning increases hydrostatic pressure and can worsen peripheral tissue perfusion. Dependency or stasis does not facilitate the arterial inflow required to oxygenate ischemic tissues. Frequent position changes are necessary to prevent localized pressure and maintain adequate circulatory flow.
C. Elevate his legs and arms above his heart when resting: This position hinders gravity-assisted arterial flow to the distal extremities, worsening ischemia. Unlike venous insufficiency, arterial disease requires the limbs to be maintained in a neutral or slightly dependent position. Elevation significantly reduces the perfusion pressure needed to reach peripheral tissues.
D. Encourage the client to engage in moderate amount of exercise: Structured walking programs stimulate the formation of collateral vessels to bypass occluded arteries. Physical activity improves oxygen extraction by the muscles and increases the pain-free walking distance. This intervention remains a cornerstone of conservative management for improving peripheral arterial circulation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today