You are assessing a client with a serum-filled blister on their heel along with partial-thickness skin loss. What is the most appropriate documentation for this condition?
Stage 3 pressure injury
Unstageable pressure injury
Stage 2 pressure injury
Stage 1 pressure injury
The Correct Answer is C
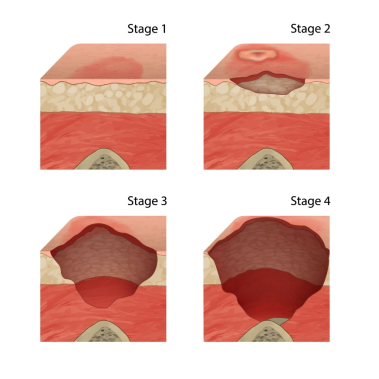
A. Stage 3 pressure injury: A Stage 3 injury involves full-thickness skin loss, extending into the subcutaneous fat.
B. Unstageable pressure injury: An Unstageable injury requires the base of the wound to be obscured by slough or eschar. This wound is visible as a blister/open ulcer.
C. Stage 2 pressure injury: A Stage 2 pressure injury is defined as partial-thickness loss of skin involving the epidermis and/or dermis. It presents as a shallow open ulcer with a red-pink wound bed, or an intact or ruptured serum-filled blister.
D. Stage 1 pressure injury: A Stage 1 injury involves intact skin with nonblanchable redness.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. Apply a warm compress to the area to improve circulation: Applying heat can increase the metabolic demands of the already compromised tissue, potentially worsening the injury.
B. Document the finding and recheck in 24 hours: A Stage 1 pressure injury requires immediate action to relieve pressure to prevent progression. Delaying intervention for 24 hours can allow the injury to worsen.
C. Massage the area gently to promote blood flow:Massaging a reddened, nonblanching area can intensify the underlying capillary and tissue damage, leading to further tissue necrosis and progression to a deeper stage.
D. Reposition the patient to relieve pressure on the heel: The nonblanchable erythema signifies deep tissue ischemia caused by unrelieved pressure. The most appropriate and critical nursing action is to eliminate the pressure immediately by repositioning the patient so the bony prominence is no longer compressed. This is the only way to reverse the ischemia.
Correct Answer is A
Explanation
A. To prevent shearing of the patient's skin: When a patient is pulled or dragged across a sheet, the deeper tissues (bone and muscle) are stationary while the skin moves, leading to shear injury—one of the primary mechanisms for Deep Tissue Pressure Injuries (DTPIs). Using a lift device raises the patient completely, eliminating this destructive shearing and friction force.
B. To make the repositioning process faster:While a lift device may be efficient, patient safety and skin protection are the clinical priorities, not speed.
C. To prevent the nurse from straining their back: This is an extremely important benefit for nurse safety and injury prevention, but the primary reason the intervention is implemented in the patient's plan of care is for the direct therapeutic benefit of protecting the patient's skin integrity.
D. To ensure the patient is positioned comfortably: This is a secondary benefit. While comfort is considered, the lift device's essential function is mechanical protection of the skin and underlying tissues.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today