A client diagnosed with schizophrenia, who has been taking antipsychotic medication for the last 5 months, presents in an emergency department (ED) with uncontrollable tongue movements, stiff neck, and difficulty swallowing. The nurse would expect the physician to recognize which condition and implement which treatment?
Neuroleptic malignant syndrome, treated by discontinuing antipsychotic medications
Agranulocytosis treated by administration of clozapine (Clozaril)
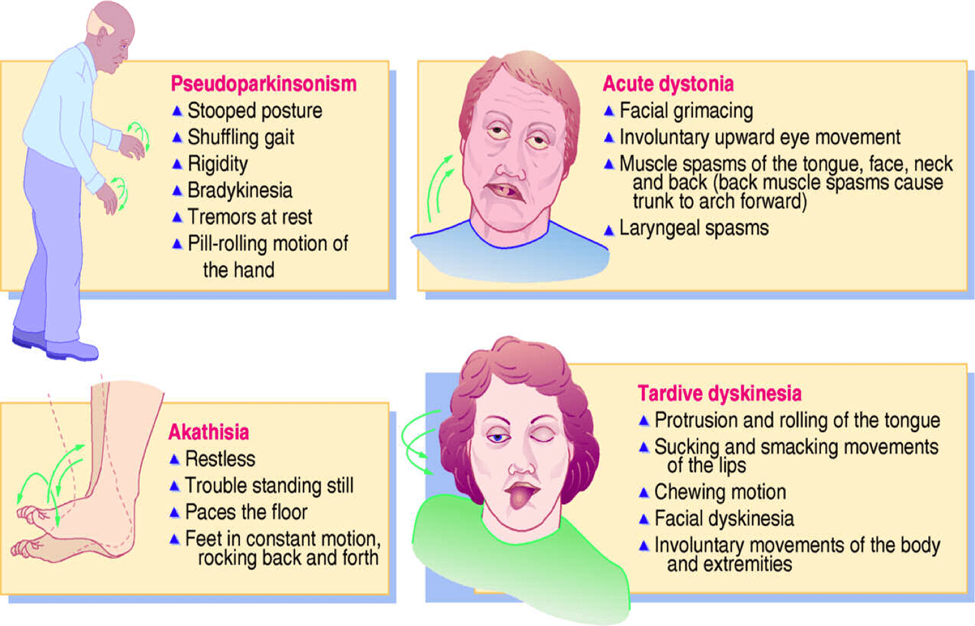
Tardive dyskinesia treated by discontinuing antipsychotic medication
Headache treated by administration of Hydrochlorothiazide
The Correct Answer is C
A. Neuroleptic malignant syndrome, treated by discontinuing antipsychotic medications: The symptoms described (uncontrollable tongue movements, stiff neck, difficulty swallowing) are more indicative of tardive dyskinesia than neuroleptic malignant syndrome. Neuroleptic malignant syndrome is characterized by hyperthermia, autonomic dysregulation, altered mental status, and generalized muscle rigidity. Treatment involves discontinuing antipsychotic medications and supportive care.
B. Agranulocytosis treated by administration of clozapine (Clozaril): Agranulocytosis is a rare but serious side effect of clozapine, not a treatment for the symptoms described. The symptoms presented are more consistent with tardive dyskinesia.
C. Tardive dyskinesia treated by discontinuing antipsychotic medication: This is the correct answer. Tardive dyskinesia is a movement disorder characterized by involuntary and abnormal movements, including tongue protrusion and facial grimacing. It can result from long-term use of antipsychotic medications, and discontinuing or reducing the dose of the antipsychotic is a primary intervention.
D. Headache treated by administration of Hydrochlorothiazide: Hydrochlorothiazide is a diuretic used to treat conditions like high blood pressure and edema, not headache or the symptoms described, which are more indicative of tardive dyskinesia.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Disturbed sensory perception: While the client is experiencing disturbed sensory perception (auditory hallucinations), the priority is to address the potential harm to others, which is better captured by the "Risk for violence: directed toward others" diagnosis.
B. Risk for violence: directed toward others: This diagnosis is the priority in this situation because the client is expressing homicidal thoughts directed toward a specific target (the president). Ensuring the safety of the client and others is the primary concern.
C. Altered thought processes: Altered thought processes may be evident in psychotic disorders, but the immediate concern is the risk of violence. Addressing altered thought processes would be part of the overall care plan, but it may not be the immediate priority in this case.
D. Risk for injury: While the client may be at risk for injury, the specific concern mentioned by the client is the potential harm to others (the president). Therefore, the "Risk for violence: directed toward others" diagnosis takes precedence.
Correct Answer is D
Explanation
A. Having an advanced degree in engineering:
While pursuing an advanced degree can be challenging, it is not inherently a source of psychological distress. It may represent a personal and professional accomplishment.
B. Attending a community center daily:
Attending a community center daily is a regular activity and may not necessarily be a source of psychological distress. It could be a positive and fulfilling aspect of one's routine.
C. Belonging to the middle-class socioeconomic group:
Belonging to the middle-class socioeconomic group is not inherently a source of psychological distress. Socioeconomic status alone does not determine psychological well-being, and being in the middle class can provide stability and resources.
D. Being the only person of their ethnicity in a school setting:
This qualifies as a source of psychological distress. Being the only person of a particular ethnicity in a school setting may lead to feelings of isolation, cultural dissonance, and a sense of being different. Such situations can contribute to psychological distress and impact mental well-being.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today