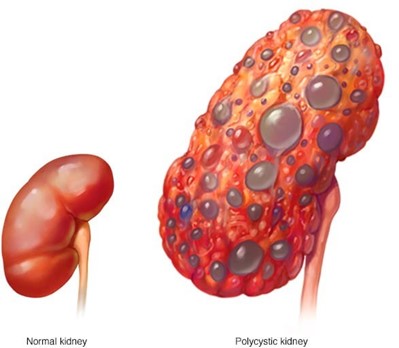
A client is being treated for chronic kidney disease (CKD). On examination, the client has an elevated blood pressure (BP) and is exhibiting changes in mental status. Which intervention in the plan of care should the practical nurse (PN) implement?
Use a cushion when sitting.
Perform range of motion exercises.
Document abdominal girth.
Weigh every morning.
The Correct Answer is D
This is the best intervention for the PN to implement because it monitors the client's fluid status and helps detect fluid overload, which can cause hypertension and neurological changes. The PN should weigh the client at the same time, on the same scale, and with the same clothing every day.
A. Using a cushion when sitting is not a priority intervention for this client and may not address the BP or mental status issues.
B. Performing range of motion exercises is not a priority intervention for this client and may not address the BP or mental status issues.
C. Documenting abdominal girth is not a priority intervention for this client and may not be an accurate indicator of fluid status.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["40"]
Explanation
The client’s 0730 finger stick glucose is 271 mg/dL. According to the sliding scale parameters, the client should receive:
Step 1: Determine the amount of insulin aspart based on the sliding scale. Since the glucose level is 271 mg/dL, which falls in the range of 270 to 300 mg/dL, the client should receive 15 units of insulin aspart.
Step 2: Add the amount of NPH insulin to the amount of insulin aspart. The client has a prescription for NPH insulin 25 units before breakfast. So, the total amount of insulin this client should receive is 25 units (NPH insulin) + 15 units (insulin aspart) = 40 units.
So, the total amount of insulin this client should receive is40 units.
Correct Answer is A
Explanation
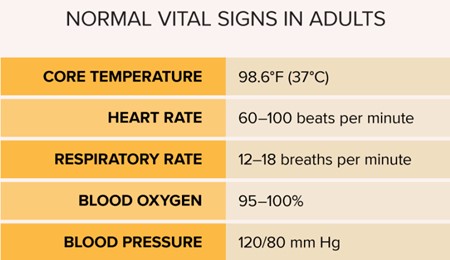
This is the most important follow-up assessment for the PN to implement because it can detect signs of bleeding, infection, or shock that may result from the unsecured surgical dressing. The PN should monitor the client's blood pressure, pulse, temperature, and respiratory rate and report any abnormal changes.
B. Fluid volume intake and output is not the most important follow-up assessment for this client and may not reflect the current status of the client's fluid balance or blood loss.
C. Volume of peripheral pulses is not the most important follow-up assessment for this client and may not be affected by the unsecured surgical dressing unless it is located on a limb or near a major artery.
D. Incisional pain scale rating is not the most important follow-up assessment for this client and may not indicate the severity or cause of the client's pain.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today