A nurse is assessing a client for manifestations of pain. Which of the following findings is an objective indicator of pain?
The client rates their pain as an 8 on a scale of 0 to 10.
The client states the pain is located on their abdomen.
The client reports a burning sensation.
The client grimaces when they move.
The Correct Answer is D
Answer: D. The client grimaces when they move.
Rationale:
A) The client rates their pain as an 8 on a scale of 0 to 10:
Pain ratings provided by the client are subjective and reflect their personal experience and perception of pain. While important for assessing pain severity, this rating is based on the client's personal report rather than observable evidence.
B) The client states the pain is located on their abdomen:
The location of pain, as reported by the client, is subjective information. It is based on the client's personal experience and cannot be objectively measured or observed by the nurse.
C) The client reports a burning sensation:
Describing the sensation of pain, such as a burning feeling, is a subjective experience. This description provides valuable information about the nature of the pain but does not serve as an objective indicator.
D) The client grimaces when they move:
Observing a grimace is an objective indicator of pain. It is a visible, physical response that the nurse can see and document, indicating that the client is experiencing discomfort or pain. Objective indicators are observable signs that can be noted by healthcare providers.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
The nurse should expect to find an increased heart rate in a client with a fever. An elevated body temperature can cause an increase in metabolic rate, which can lead to an increase in heart rate. This is a normal physiological response to fever and helps the body to generate heat and fight off infection.
Correct Answer is A
Explanation
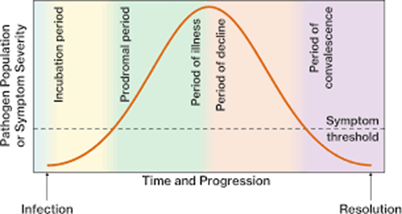
The client is likely experiencing the acute illness stage of infection, which is characterized by the appearance of specific signs and symptoms of the disease. During this stage, the individual may feel ill and exhibit symptoms such as sneezing, productive cough, muscle aches, headache, and fever.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today