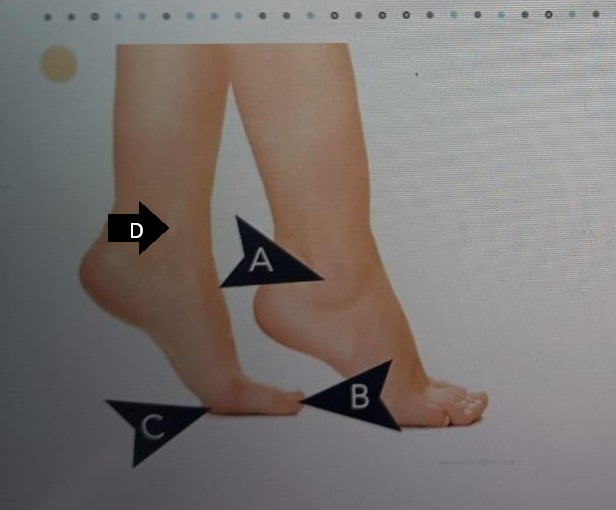
A nurse is caring for a client who has chronic venous insufficiency. Which of the following areas should the nurse assess for the presence of a venous ulcer?
A
B
C
D
The Correct Answer is D
Rationale:
A. This area is the lateral side of the the heel and is more commonly affected by arterial ulcers or pressure injuries. It is not the typical location for ulcers caused by venous insufficiency.
B. This area is the area on the tip of toes and is not a typical site for venous ulcers. Ulcers in this location are commonly arterial or diabetic ulcers.
C. This area is the area on the sole of the feet at the base of the big toe and is not a typical site for venous ulcers.
D. This area is the medial malleolus, just above the inner ankle, which is the most common site for venous ulcers. Chronic venous insufficiency leads to venous stasis and increased pressure in this region, causing skin breakdown and ulceration.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Rationale:
A. Dependent edema: This occurs due to fluid buildup in the peripheral tissues, which is typically caused by right-sided heart failure. It reflects systemic venous congestion rather than pulmonary issues associated with left-sided failure.
B. Jugular distention: Jugular venous distention is a sign of increased central venous pressure and is more often associated with right-sided heart failure, not the pulmonary congestion seen in left-sided failure.
C. Weight gain: Weight gain from fluid retention is more indicative of right-sided heart failure, which causes systemic congestion; it is not a primary manifestation of left-sided heart failure.
D. Frothy sputum: Frothy, often pink-tinged sputum results from pulmonary edema caused by left-sided heart failure. Blood backs up into the lungs due to poor left ventricular function, leading to fluid leakage into the alveoli.
Correct Answer is D
Explanation
Rationale:
A. Decreased WBC count: Bacterial meningitis causes an inflammatory response, leading to an increased WBC count in the cerebrospinal fluid (CSF), not a decrease. Elevated WBCs indicate the body is fighting infection in the central nervous system.
B. Increased glucose: CSF glucose levels are typically decreased because bacteria consume glucose and impair its transport across the blood-brain barrier. The presence of leukocytes and pathogens in the CSF also contributes to glucose depletion. Elevated glucose is not characteristic of this condition.
C. Clear cerebrospinal fluid: CSF in bacterial meningitis is usually cloudy or turbid due to the accumulation of white blood cells, protein, and bacteria. The change in appearance reflects the severity of the infection and is one of the classic diagnostic signs. Clear CSF would be more consistent with normal or viral findings.
D. Increased protein: A hallmark of bacterial meningitis is elevated CSF protein levels due to increased permeability of the blood-brain barrier and the presence of bacterial and inflammatory proteins. This is an expected finding.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today