A nurse is caring for an infant who has gastroenteritis.
Which of the following assessment findings should the nurse report to the provider?
Sunken fontanels and dry mucous membranes.
Temperature 38° C (100.4° F) and pulse rate 124/min.
Decreased appetite and irritability.
Pale and a 24-hr fluid deficit of 30 mL.
The Correct Answer is A
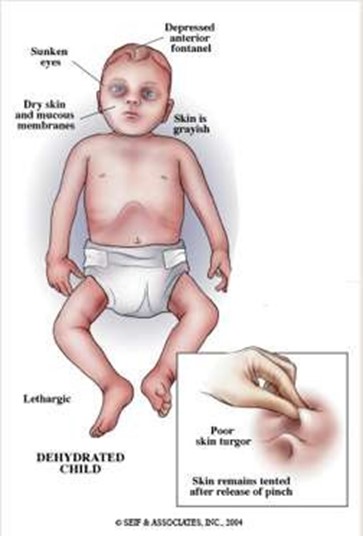
These are signs of severe dehydration in an infant, which can be life-threatening and should be reported to the provider immediately. The infant may need intravenous fluids and electrolytes to restore hydration and prevent complications.
Choice B is wrong because a temperature of 38° C (100.4° F) and a pulse rate of 124/min are not abnormal for an infant and do not indicate severe dehydration. These are common findings in an infant who has gastroenteritis, which is an inflammation of the stomach and intestines caused by a virus, bacteria, or parasite.
Choice C is wrong because decreased appetite and irritability are also common findings in an infant who has gastroenteritis, but they do not indicate severe dehydration. The nurse should encourage oral rehydration with fluids such as breast milk, formula, or oral electrolyte solution.
Choice D is wrong because pale skin and a 24-hr fluid deficit of 30 mL are not signs of severe dehydration in an infant.
A fluid deficit of 30 mL is less than 1 oz and is not significant for an infant who weighs about 10 kg (22 lbs). A fluid deficit of more than 10% of body weight would indicate severe dehydration.
Normal ranges for vital signs in infants are as follows:
• Temperature: 36.5° C to 37.5° C (97.7° F to 99.5° F)
• Pulse rate: 100 to 160/min
• Respiratory rate: 30 to 60/min
• Blood pressure: 65/41 to 100/50 mm Hg
Normal ranges for fluid intake and output in infants are as follows:
• Fluid intake: 100 to 150 mL/kg/day
• Fluid output: 1 to 2 mL/kg/hr
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
The correct answer is c. Remove the cap and place it sterile-side up on a clean surface.
Choice A rationale:
Placing sterile gauze over areas of spilled solution within the sterile field is incorrect. If solution is spilled within the sterile field, the entire field should be considered contaminated and a new sterile field should be set up
Choice B rationale:
Holding the irrigation solution bottle with the label facing away from the palm of the hand is incorrect. The label should face the palm of the hand to avoid contamination of the sterile field
Choice C rationale:
Removing the cap and placing it sterile-side up on a clean surface is correct. This ensures that the sterile side of the cap remains sterile and can be used to recap the bottle after pouring the solution
Choice D rationale:
Holding the bottle in the center of the sterile field when pouring the solution is incorrect. The bottle should be held over the edge of the sterile field to avoid contamination of the field if solution spills
Correct Answer is ["C","E"]
Explanation
A urine culture is indicated for the client who has lower back pain and pinkish vaginal discharge, as these symptoms may suggest a urinary tract infection (UTI). A urine culture can identify the causative organism and guide the appropriate antibiotic therapy.
Phenazopyridine is a urinary analgesic that can relieve pain, burning, and urgency associated with a UTI. However, it requires a provider prescription and should not be used for more than two days.
A vaginal culture is not necessary for this client, as the vaginal discharge is likely due to the cervical changes during labor. A vaginal culture may be indicated for clients who have signs of vaginitis, such as itching, odor, or abnormal color of the discharge.
Obtaining a provider prescription for antibiotics is premature for this client, as the urine culture results are not available yet. Antibiotics should be prescribed based on the sensitivity of the organism causing the UTI.
Ibuprofen 600 mg every 6 hr for mild to moderate pain is not appropriate for this client, as it may interfere with uterine contractions and prolong labor. Ibuprofen is also contraindicated in the third trimester of pregnancy due to the risk of premature closure of the ductus arteriosus in the fetus. The nurse should use nonpharmacological methods to relieve the client’s back pain, such as massage, heat, or position changes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today