A nurse is performing a focused assessment for a client's vision. What visual assessment is the nurse making when she extends her hand for the client to shake?
Depth perception
Peripheral vision
Color deficit
Double vision
The Correct Answer is B
Choice A Reason: Depth perception is the ability to judge the distance and position of objects in three-dimensional space. Depth perception is assessed by asking the client to touch the tip of a pen or pencil held by the nurse, or by using a stereopsis test.
Choice B Reason: Peripheral vision is the ability to see objects and movements outside the direct line of vision. Peripheral vision is assessed by asking the client to shake the hand of the nurse, who stands at an angle to the client's side, or by using a confrontation test.
Choice C Reason: Color deficit is the inability to distinguish certain colors or shades of colors. Color deficit is assessed by asking the client to identify numbers or shapes on a color plate test, such as the Ishihara test.
Choice D Reason: Double vision is the perception of two images of a single object. Double vision is assessed by asking the client to cover one eye and look at an object, then switch eyes and compare the images, or by using a cover-uncover test.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
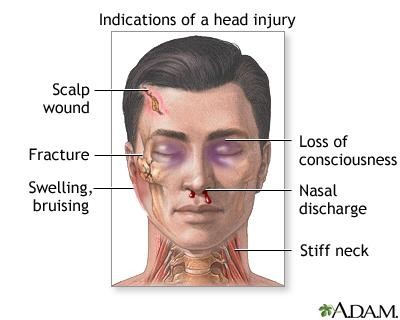
Choice A Reason: This is the correct choice because driving a motorcycle is a high-risk activity that can expose the client to head trauma, especially if they do not wear a helmet. Traumatic brain injury (TBI) is a condition where the brain is damaged by an external force, such as a collision, fall, or assault.
Choice B Reason: This is incorrect because having high blood pressure is not a direct risk factor for traumatic brain injury. High blood pressure can increase the risk of stroke, which is a condition where the brain is damaged by an internal cause, such as a blood clot or hemorrhage.
Choice C Reason: This is incorrect because smoking and having a family history of brain cancer are not risk factors for traumatic brain injury. Smoking and genetic factors can increase the risk of developing brain tumors, which are abnormal growths of cells in the brain.
Choice D Reason: This is incorrect because golfing and driving a golf cart are low-risk activities that do not pose a significant threat to the client's head. Golfing and driving a golf cart may cause minor injuries, such as sprains, strains, or bruises, but not traumatic brain injury.
Correct Answer is D
Explanation
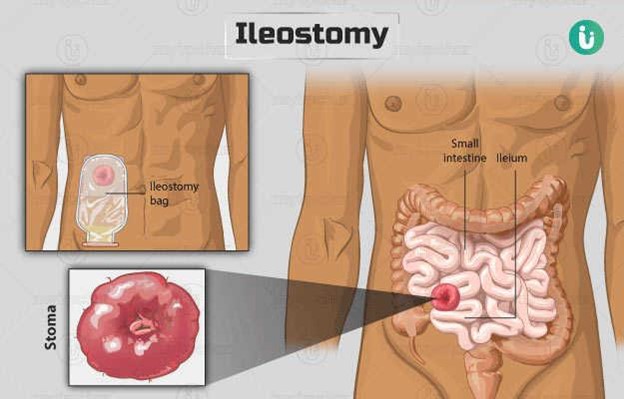
Choice A Reason: This is incorrect because intestinal obstruction is not a common complication of ileostomy surgery. An ileostomy is a surgical opening in the abdomen that connects the end of the small intestine (ileum) to a pouch or bag outside the body. This allows stool to bypass the colon and rectum. Intestinal obstruction can occur if there is a blockage or narrowing in any part of the digestive tract, but it is more likely to affect the colon than the ileum.
Choice B Reason: This is incorrect because folate deficiency is not a common complication of ileostomy surgery. Folate is a vitamin that is essential for DNA synthesis and cell division. Folate is mainly absorbed in the jejunum, which is the middle part of the small intestine. An ileostomy does not affect the jejunum, so it does not interfere with folate absorption.
Choice C Reason: This is incorrect because malabsorption of fat is not a common complication of ileostomy surgery. Fat is digested and absorbed in both the small and large intestine. An ileostomy does not affect fat digestion, but it may reduce fat absorption by decreasing the transit time and surface area of the intestine. However, this is usually not significant enough to cause malabsorption symptoms.
Choice D Reason: This is correct because fluid and electrolyte imbalance is a common complication of ileostomy surgery. Fluid and electrolytes are mainly absorbed in the colon, which is bypassed by an ileostomy. This can result in increased fluid and electrolyte loss through stool, especially sodium and potassium. This can lead to dehydration, hypotension, weakness, cramps, or arrhythmias.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today