A nurse is preparing to review discharge instructions with a client who reports having hearing loss. Which of the following actions should the nurse plan to take?
Stand next to the client when speaking.
Guide the client away from background noise.
Provide a copy of the instructions printed in Braille.
Repeat any phrases that the client misunderstands.
Correct Answer : A,B,D
Choice A Reason: This is a correct choice. Standing next to the client when speaking is an action that the nurse should plan to take, as it helps the client hear better and see the nurse's facial expressions and lip movements. The nurse should also speak clearly and slowly, use simple words and sentences, and avoid covering their mouth.
Choice B Reason: This is a correct choice. Guiding the client away from background noise is an action that the nurse should plan to take, as it reduces distractions and interference with hearing. The nurse should also choose a well-lit and quiet place for communication and turn off any unnecessary devices or appliances.
Choice C Reason: This is an incorrect choice. Providing a copy of the instructions printed in Braille is not an action that the nurse should plan to take, as it is not helpful for clients with hearing loss. Braille is a system of raised dots that represents letters and numbers for people who are blind or visually impaired. The nurse should provide a copy of the instructions printed in large font or use pictures or diagrams to supplement verbal information.
Choice D Reason: This is a correct choice. Repeating any phrases that the client misunderstands is an action that the nurse should plan to take, as it ensures comprehension and clarification of important information. The nurse should also ask open-ended questions, encourage feedback, and summarize key points at the end of the conversation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
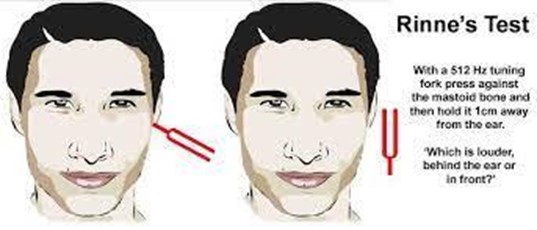
Choice A Reason: This is incorrect because earphones are not used in the Rinne test. The Rinne test compares air conduction and bone conduction of sound using a tuning fork.
Choice B Reason: This is incorrect because electrodes are not used in the Rinne test. Electrodes are used in electroencephalography (EEG), which measures brain activity.
Choice C Reason: This is incorrect because a probe is not used in the Rinne test. A probe is used in tympanometry, which measures the pressure and mobility of the eardrum.
Choice D Reason: This is correct because a tuning fork is used in the Rinne test. The tuning fork is placed on the mastoid process behind the ear and then moved near the ear canal to compare the sound perception.
Correct Answer is ["A","B","C","D","E"]
Explanation
Choice A Reason: This is correct because clinical obesity is a risk factor for metabolic syndrome. Clinical obesity is defined by having a body mass index (BMI) of 30 or higher, or a waist circumference of more than 40 inches for men or 35 inches for women. Obesity can increase insulin resistance and inflammation, which can lead to metabolic syndrome.
Choice B Reason: This is correct because elevated blood pressure is a risk factor for metabolic syndrome. Elevated blood pressure is defined by having a systolic blood pressure of 130 mm Hg or higher, or a diastolic blood pressure of 85 mm Hg or higher. High blood pressure can damage the blood vessels and increase the risk of cardiovascular disease, which is associated with metabolic syndrome.
Choice C Reason: This is correct because high triglycerides are a risk factor for metabolic syndrome. Triglycerides are a type of fat that circulates in the blood and provides energy for the cells. High triglycerides are defined by having a level of 150 mg/dL or higher. High triglycerides can increase the risk of fatty liver disease and pancreatitis, which are related to metabolic syndrome.
Choice D Reason: This is correct because hypercholesterolemia is a risk factor for metabolic syndrome. Hypercholesterolemia is defined by having a total cholesterol level of 200 mg/dL or higher, or a low-density lipoprotein (LDL) cholesterol level of 100 mg/dL or higher. LDL cholesterol is also known as "bad" cholesterol because it can build up in the arteries and cause plaque formation and narrowing, which can lead to cardiovascular disease and metabolic syndrome.
Choice E Reason: This is correct because hyperglycemia is a risk factor for metabolic syndrome. Hyperglycemia is defined by having a fasting blood glucose level of 100 mg/dL or higher, or a hemoglobin A1c level of 5.7% or higher. Hemoglobin A1c is a measure of average blood glucose over three months. Hyperglycemia can indicate impaired glucose metabolism and insulin resistance, which are hallmarks of metabolic syndrome.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today