A nurse is reviewing the medical record of a client who is requesting an oral contraceptive.
Which of the following findings should the nurse identify as a contraindication to the use of oral contraceptives?
History of renal calculus
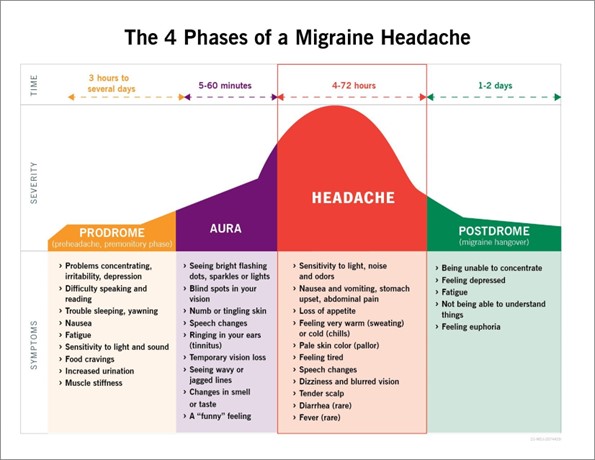
Migraines with aura
BMI of 25
History of cholecystectomy
The Correct Answer is B
b. Migraines with aura.
Explanation:
Migraines with aura are considered a contraindication to the use of oral contraceptives. Auras are neurological symptoms that occur before or during migraines and can include visual disturbances, sensory changes, or speech difficulties. Women who experience migraines with aura have an increased risk of ischemic stroke when taking oral contraceptives. Therefore, it is important to identify this condition as a contraindication and explore alternative contraceptive options for the client.
The other options (a. History of renal calculus, c. BMI of 25, d. History of cholecystectomy) are not contraindications to the use of oral contraceptives.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
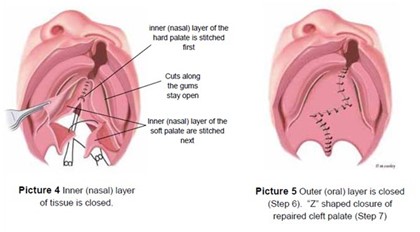
The nurse should include maintaining elbow restraints on the infant in the plan of care following cleft palate repair. This helps to prevent the infant from touching their surgical site and disrupting the healing process.
a) Allowing the infant to have soft foods may be appropriate, but it is not the highest priority. The infant's diet should be determined by the provider and based on the infant's individual needs.
c) Instructing the parents to feed the infant with a spoon may be appropriate, but it is not the highest priority. The infant's feeding method should be determined by the provider and based on the infant's individual needs.
d) Telling the parents to avoid brushing the infant's teeth for two weeks may be appropriate, but it is not the highest priority. The infant's oral care should be determined by the provider and based on the infant's individual needs.
Correct Answer is D
Explanation
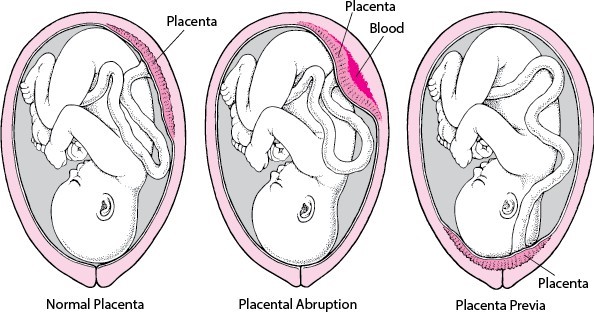
Placenta previa is a condition where the placenta partially or completely covers the opening of the cervix. One of the hallmark signs of placenta previa is painless vaginal bleeding, typically bright red in color. This bleeding can occur spontaneously or during activities that put pressure on the uterus, such as sexual intercourse or physical exertion.
A rigid abdomen is not typically associated with placenta previa. It may indicate other conditions, such as peritonitis or abdominal muscle rigidity, but it is not a characteristic finding of placenta previa.
Persistent uterine contractions are not typically associated with placenta previa. Placenta previa is more commonly associated with painless bleeding rather than contractions. However, if placenta previa is complicated by other factors, such as placental abruption, contractions and abdominal pain may be present.
Fetal movement is not directly related to placenta previa. Fetal movement can vary from person to person and does not specifically indicate placenta previa. However, it is important for the nurse to assess fetal well-being in clients with placenta previa as bleeding can impact the oxygen supply to the fetus.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today