A nurse is teaching a client who has a new diagnosis of diabetes mellitus about foot care.
Which of the following instructions should the nurse include in the teaching?
Soak feet twice daily.
Wear clean cotton socks every day.
Round the edges of toenails when trimming.
Use moisturizing lotion between the toes.
undefined
The Correct Answer is B
The correct answer is choice B. Wear clean cotton socks every day.
This is because cotton socks can help keep the feet dry and prevent infections. Wearing clean socks every day can also prevent blisters and injuries from friction.
Choice A is wrong because soaking feet twice daily can make the skin too soft and prone to injury. It can also wash away natural oils that protect the skin.
Choice C is wrong because rounding the edges of toenails when trimming can cause ingrown nails, which can lead to infection and pain. Toenails should be trimmed straight across and filed smooth.
Choice D is wrong because using moisturizing lotion between the toes can create a moist environment that promotes fungal growth. Moisturizing lotion should be applied to the rest of the feet, but not between the toes.
Some other foot care guidelines for people with diabetes are:
- Inspect your feet daily and look for signs of injury, such as scrapes, cuts, blisters, etc.
- Wash your feet every day in warm water with mild soap.
Hot water and harsh soaps can damage your skin. Check the water temperature with your fingers or elbow before putting your feet in.
- Don’t walk barefoot.
Protect your feet from heat and cold. Wear appropriate fitting shoes to avoid injury and blisters.
- See a doctor to remove corns or calluses (don’t do it yourself). Don’t use chemical wart removers, razor blades, corn plasters, or liquid corn or callus removers.
- Don’t sit with your legs crossed or stand in one position for long periods of time.
- See your doctor regularly for foot exams and report any problems or changes in your feet.
References:
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures.
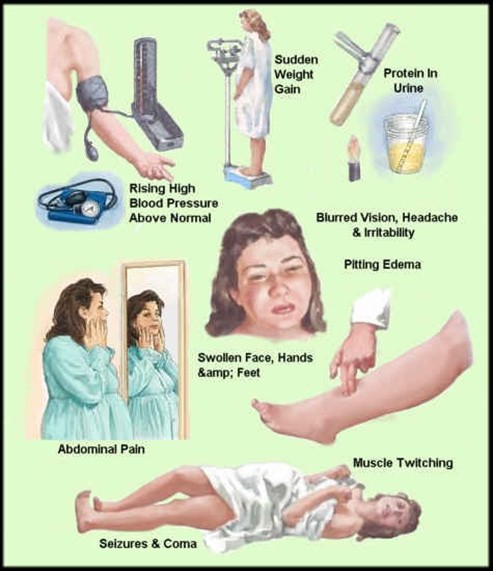
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
Choice A, bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
Choice B, urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
Choice D, faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
This can happen during pregnancy due to the dilation of blood vessels and the increased blood volume. It can be prevented by rising slowly, drinking enough fluids, and avoiding prolonged standing.
Correct Answer is {"dropdown-group-1":"C","dropdown-group-2":"C"}
Explanation
The nurse should first administer oxygen at 2 L/min via nasal cannula because the client has signs of hypoxemia (low oxygen saturation) and respiratory distress (increased respiratory rate) that may worsen the chest pain and myocardial ischemia. Oxygen therapy can help improve oxygen delivery to the heart muscle and reduce the workload of the heart.
The nurse should then administer sublingual nitroglycerin as prescribed because nitroglycerin is a vasodilator that can help relieve chest pain by dilating the coronary arteries and improving blood flow to the heart. Nitroglycerin can also lower blood pressure and reduce cardiac preload and afterload, which can decrease myocardial oxygen demand.
Other choices:
• Prepare the client for cardiac catheterization: This may be a later intervention if the chest pain persists or if the client has a confirmed myocardial infarction, but it is not the first priority for the nurse. Cardiac catheterization is an invasive procedure that involves inserting a catheter into a large artery and advancing it to the coronary arteries to visualize any blockages or stenosis. The procedure may also involve angioplasty or stent placement to restore blood flow to the affected area.
• Request a prescription for an increase in statin: This may be a long-term intervention to lower the client’s LDL cholesterol and prevent further plaque formation in the coronary arteries, but it is not an immediate intervention for chest pain. Statins are lipid-lowering drugs that can reduce the risk of cardiovascular events in clients with CAD, but they do not have a direct effect on chest pain or myocardial ischemia.
• Check a STAT cardiac troponin: This may be a diagnostic test to confirm or rule out a myocardial infarction, but it is not an intervention for chest pain. Cardiac troponin is a protein that is released into the bloodstream when there is damage to the heart muscle. Elevated levels of cardiac troponin indicate a myocardial infarction or other cardiac injury.
• Request a prescription for a beta-blocker: This may be an adjunctive therapy to reduce chest pain and prevent complications, but it is not the first-line intervention for chest pain. Beta-blockers are drugs that block the effects of adrenaline on the heart and blood vessels, which can lower heart rate, blood pressure, and myocardial oxygen demand. Beta-blockers can also prevent arrhythmias and reduce mortality in clients with CAD.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today