A patient with a head injury opens his eyes to verbal stimulation, shouts out when stimulated, and does not respond to a verbal command to move but attempts to push away a painful stimulus. How would the nurse record the patient's Glasgow Coma Scale score?
9
11
15
13
The Correct Answer is A
Choice A Reason: This is correct because the patient's Glasgow Coma Scale score is 9. The Glasgow Coma Scale is a tool that assesses the level of consciousness of a patient with a head injury by measuring three parameters: eye opening, verbal response, and motor response. The patient's eye opening score is 3 (opens eyes to verbal command), verbal response score is 4 (confused speech), and motor response score is 2 (withdraws from pain). The total score is the sum of these three scores, which is 9.
Choice B Reason: This is incorrect because the patient's Glasgow Coma Scale score is not 11. To get a score of 11, the patient would need to have a higher motor response score, such as 4 (withdraws to touch) or 5 (localizes to pain).
Choice C Reason: This is incorrect because the patient's Glasgow Coma Scale score is not 15. To get a score of 15, the patient would need to have the highest scores for all three parameters, such as 4 (opens eyes spontaneously), 5 (oriented speech), and 6 (obeys commands).
Choice D Reason: This is incorrect because the patient's Glasgow Coma Scale score is not 13. To get a score of 13, the patient would need to have a higher verbal response score, such as 5 (oriented speech).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: This is correct because the lesion on the child's head is most likely a hemangioma, which is a benign tumor of blood vessels that appears as a red or purple mark on the skin. Hemangiomas are common in newborns and usually grow during the first year of life, then shrink and fade over several years. The nurse should reassure the client that hemangiomas are harmless and do not require treatment unless they interfere with vision, breathing, or feeding.
Choice B reason: This is incorrect because the lesion on the child's head will not spread, but rather grow and shrink within a limited area. The nurse should not alarm the client by suggesting that the lesion will spread to other parts of the body or become malignant. The nurse should explain that hemangiomas are not contagious or infectious and do not affect the child's overall health or development.
Choice C reason: This is incorrect because the lesion on the child's head is not caused by scarring from the birth process, but rather by abnormal growth of blood vessels in the skin. The nurse should not confuse or misinform the client about the cause of the lesion. The nurse should explain that hemangiomas are not related to trauma, infection, or genetics, but rather to unknown factors that influence blood vessel formation during fetal development.
Choice D reason: This is incorrect because the lesion on the child's head is not a precancerous lesion and does not need a referral to a dermatologist. The nurse should not scare or mislead the client by suggesting that the lesion is a sign of cancer or requires further evaluation or treatment. The nurse should explain that hemangiomas are benign and usually resolve on their own without any complications or sequelae.

Correct Answer is D
Explanation
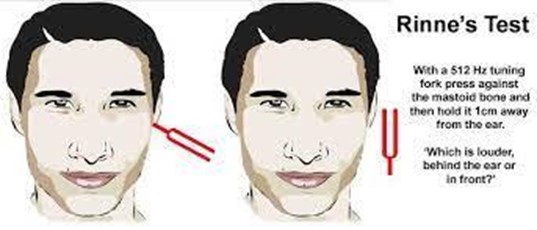
Choice A Reason: This is incorrect because earphones are not used in the Rinne test. The Rinne test compares air conduction and bone conduction of sound using a tuning fork.
Choice B Reason: This is incorrect because electrodes are not used in the Rinne test. Electrodes are used in electroencephalography (EEG), which measures brain activity.
Choice C Reason: This is incorrect because a probe is not used in the Rinne test. A probe is used in tympanometry, which measures the pressure and mobility of the eardrum.
Choice D Reason: This is correct because a tuning fork is used in the Rinne test. The tuning fork is placed on the mastoid process behind the ear and then moved near the ear canal to compare the sound perception.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today