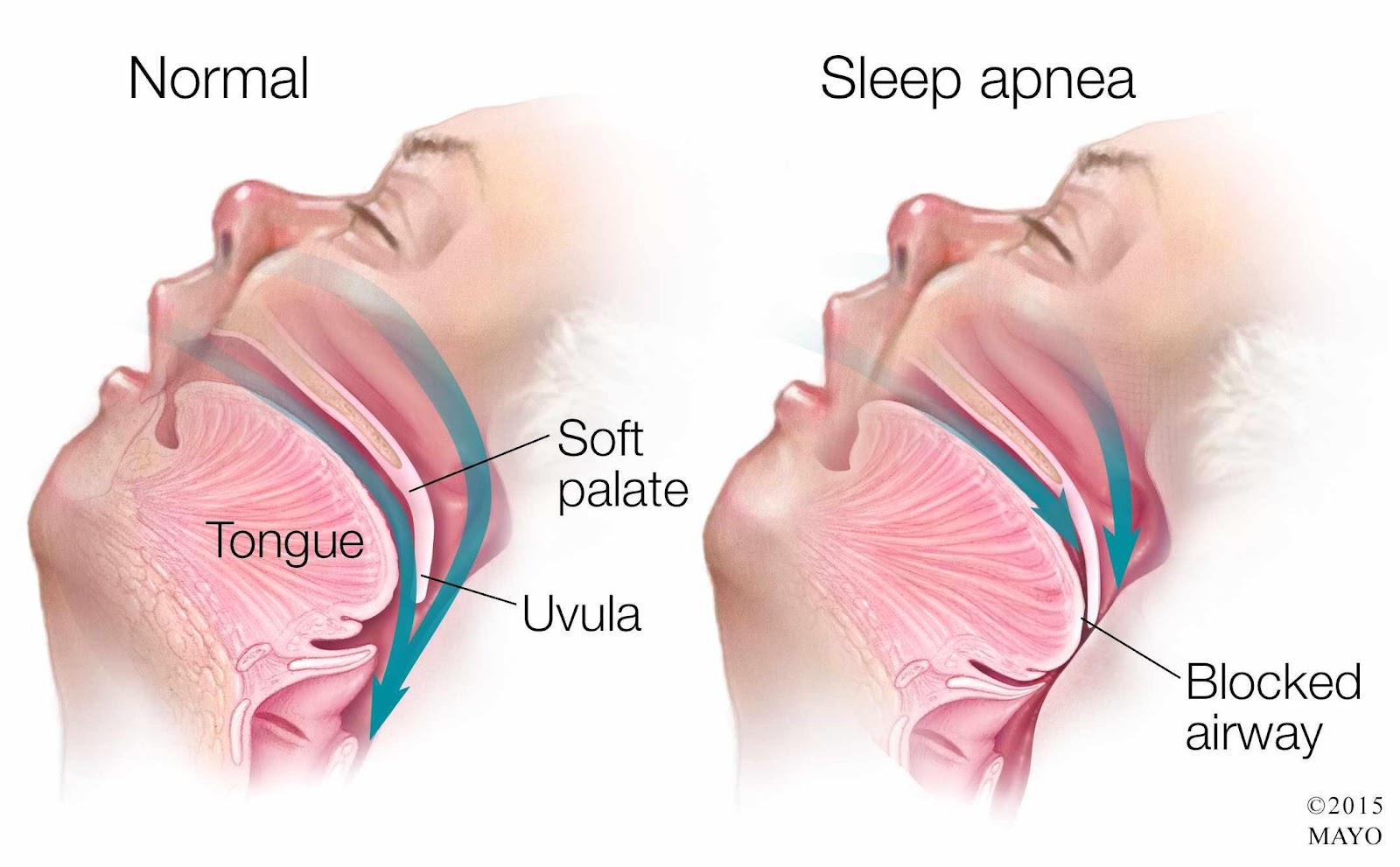
The nurse administers morphine to a client for chest pain who also has obstructive sleep apnea (OSA). Which intervention is most important for the nurse to implement before leaving the client alone?
Lift and lock the side rails in place.
Apply the client's positive airway pressure device.
Elevate the head of the bed to a 45-degree angle.
Remove dentures or other oral appliances.
The Correct Answer is B
Choice A Reason: This is incorrect because lifting and locking the side rails in place is a standard safety measure for all clients, but it does not address the specific risk of respiratory depression caused by morphine and OSA.
Choice B Reason: This is correct because applying the client's positive airway pressure device can help maintain airway patency and prevent hypoxia and hypercapnia, which are common complications of OSA and opioid use.
Choice C Reason: This is incorrect because elevating the head of the bed to a 45-degree angle can help reduce chest pain and dyspnea, but it does not prevent airway obstruction or respiratory depression.
Choice D Reason: This is incorrect because removing dentures or other oral appliances can help prevent aspiration, but it does not affect the client's breathing pattern or oxygenation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This is incorrect because decreasing the flow rate to 1 L/minute can compromise the client's oxygenation and worsen hypoxia. The client's oxygen saturation level is below the normal range of 95% to 100%.
Choice B Reason: This is correct because placing padding around the cannula tubing can prevent pressure ulcers and skin breakdown caused by friction and irritation from the tubing.
Choice C Reason: This is incorrect because applying lubricant to the cannula tubing can increase the risk of infection and inflammation of the nasal mucosa. Lubricant should be applied sparingly to the nares only if needed.
Choice D Reason: This is incorrect because discontinuing the use of the nasal cannula can endanger the client's life and cause respiratory failure. The client needs supplemental oxygen to maintain adequate oxygenation.

Correct Answer is B
Explanation
Choice A Reason: This is incorrect because explaining that alternative treatment options may be helpful can be insensitive and unrealistic, as it may raise false hopes or imply that the husband's condition is not serious.
Choice B Reason: This is correct because encouraging the wife to share her feelings can help her cope with her grief and express her emotions in a supportive environment. The nurse should use active listening and empathic responses.
Choice C Reason: This is incorrect because offering reassurance that she is not alone can be dismissive and invalidating, as it may minimize her feelings or imply that she should not feel lonely.
Choice D Reason: This is incorrect because reminding her that her husband may still live a long time can be dishonest and inappropriate, as it may contradict the medical prognosis or imply that she should not prepare for his death.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today