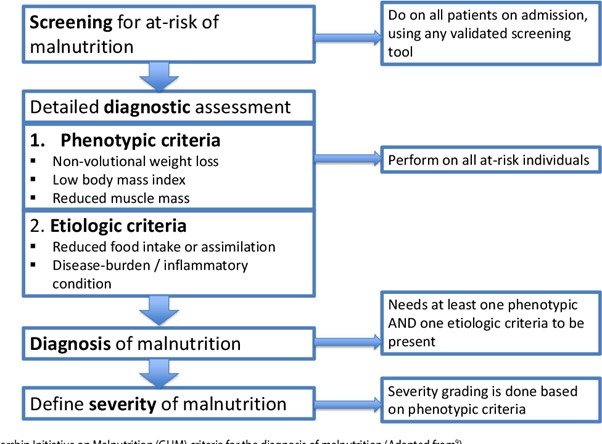
The nurse is caring for a client who has been diagnosed with malnutrition. Which finding supports the medical diagnosis?
Body mass index (BMI) of 17.
Decrease in the appetite.
Dry mucosal membranes.
Weight of 227 pounds (103 kg).
The Correct Answer is A
Choice A
Body mass index (BMI) of 17 is the correct finding. A low Body Mass Index (BMI) is a common indicator of malnutrition. BMI is a measurement that considers a person's weight in relation to their height. A BMI of 17 suggests that the person is underweight, which can be indicative of malnutrition. Malnutrition is characterized by inadequate intake of calories, protein, vitamins, and minerals that are essential for maintaining health and well-being.
Choice B
Decrease in appetite is not correct finding. While a decrease in appetite might contribute to malnutrition, it's a symptom rather than a definitive indicator.
Choice C
Dry mucosal membranes are not the correct finding. Dry mucosal membranes can be related to dehydration or other conditions, but they are not specific enough to confirm malnutrition on their own.
Choice D
Weight of 227 pounds (103 kg) is not the correct finding. This weight is not necessarily indicative of malnutrition on its own. It's important to consider the individual's height, BMI, and other factors when assessing malnutrition.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A
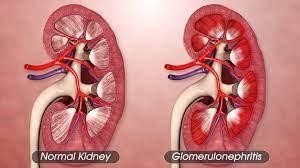
Following low carbohydrate diet with low glycaemic index foods is incorrect. This recommendation is not specifically related to the management of glomerulonephritis. While managing carbohydrate intake might be relevant for individuals with diabetes, it's not the primary focus for someone with kidney inflammation.
Choice B
Eating a high protein diet three times a day is incorrect: While protein is important for overall health and recovery, a high protein diet might not be the best recommendation for someone with compromised kidney function. Excessive protein intake could potentially put additional strain on the kidneys.
Choice C
Avoiding foods high in potassium is correct. Examples of foods high in potassium that the client should be cautious about include bananas, oranges, potatoes, tomatoes, spinach, and other fruits and vegetables. Glomerulonephritis is a condition involving inflammation of the glomeruli in the kidneys, which can affect kidney function and the regulation of electrolytes, including potassium. In glomerulonephritis, the kidneys might have difficulty filtering and excreting excess potassium, leading to a potential build-up of potassium in the blood (hyperkalaemia).
Choice D
Restricting sodium rich foods and excessive oral fluids is incorrect. This recommendation aligns more closely with managing fluid retention and blood pressure, which can be relevant for individuals with kidney issues. However, the primary concern in glomerulonephritis is often potassium balance, making the recommendation to avoid high potassium foods more pertinent.
Correct Answer is D
Explanation
Correct answer: D
Choice A
Urinary ketones are not most important. Monitoring urinary ketones can provide information about the utilization of glucose and fat as energy sources. However, it is not the primary lab value to monitor in TPN administration.
Choice B
Serum protein is not most important. Monitoring serum protein levels is important to assess nutritional status, but it might not be as immediate a concern as serum osmolarity.
Choice C
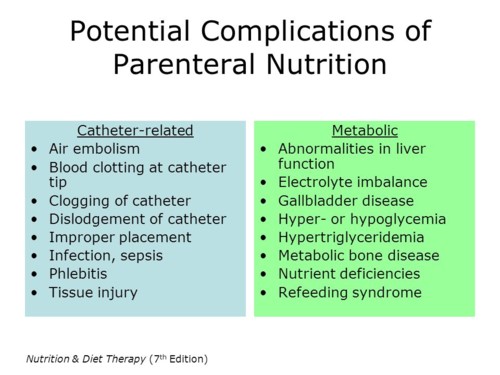
Serum osmolarity reflects the concentration of particles (such as electrolytes, glucose, and other solutes) in the blood. Monitoring serum osmolarity is importantto prevent complications related to fluid and electrolyte imbalances that can arise from the administration of TPN.Blood glucose levels (option D) are more critical because TPN can significantly impact glucose metabolism
Choice D
When caring for a client receiving total parenteral nutrition (TPN), the nurse’spriorityis tomonitor blood glucose levels. TPN can affect blood glucose, and observing for signs of hyperglycemia or hypoglycemia is crucial.Additionally, administering insulin as directed based on blood glucose levels is essential.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today