The nurse is doing a neurologic assessment on a 2-month-old infant after a car accident. Moro, tonic neck, and withdrawal reflexes are present. The nurse should recognize that these reflexes are:
Symptomatic of decorticate posturing
Symptomatic of decerebrate posturing
Indicators of severe brain damage
Normal Findings
The Correct Answer is D
Reflexes play a crucial role in evaluating the neurological status of infants.
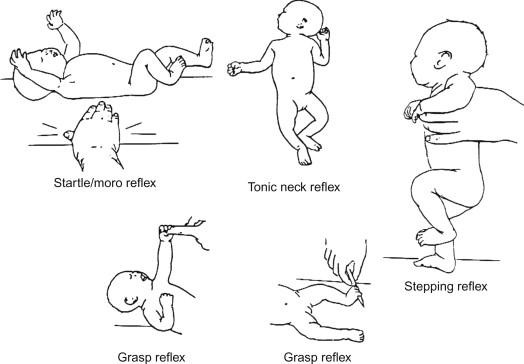
Moro reflex: Also known as the startle reflex, the Moro reflex is a normal response in infants. It occurs when an infant is startled by a sudden noise or movement. The baby responds by extending their arms and legs, followed by a quick contraction. This reflex usually disappears around 4-6 months of age.
Tonic neck reflex (fencer's reflex): This reflex involves turning an infant's head to one side, causing the arm on that side to extend and the opposite arm to flex. It's a normal reflex that typically disappears around 4-6 months of age.
Withdrawal reflex: The withdrawal reflex is a normal response to a stimulus, such as touching a baby's foot with a cold object. The baby will pull their leg away in response to the stimulus.
Symptomatic of decorticate or decerebrate posturing (options A and B):
Decorticate and decerebrate posturing are abnormal postures seen in individuals with severe brain damage or injury. Decorticate posturing involves the arms being flexed and held close to the body, while decerebrate posturing involves the arms being extended and the wrists being pronated. These reflexes are typically indicative of significant neurological dysfunction and are not expected in a 2-month-old infant after a car accident.
Indicators of severe brain damage (option C):
The reflexes described (Moro, tonic neck, and withdrawal reflexes) are not indicative of severe brain damage in a 2-month-old infant. These reflexes are normal for an infant of this age and are part of their typical neurological development.
Normal findings (option D):
The reflexes described are normal findings in a 2-month-old infant and are expected as part of their developmental milestones.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Elevate the head of the bed 15 to 30 degrees with head maintained a midline position.
Correct Explanation: This intervention is appropriate for a child with an acute head injury.
Explanation: Elevating the head of the bed helps reduce intracranial pressure by facilitating venous drainage from the head. However, it's important to keep the head in a midline position to prevent neck flexion, which can obstruct venous flow. Elevating the head 15 to 30 degrees is a standard approach for managing intracranial pressure in patients with head injuries.
B. Maintain an active stimulating environment.
Incorrect Explanation: Maintaining an active stimulating environment is not suitable for a child with an acute head injury.
Explanation: A child with an acute head injury should be in a quiet and calm environment. Overstimulation can worsen the condition by increasing intracranial pressure. It's important to minimize stimuli to allow the brain to heal.
C. Perform active chest percussion and suctioning every 1 to 2 hours.
Incorrect Explanation: Chest percussion and suctioning are not relevant interventions for an acute head injury.
Explanation: Active chest percussion and suctioning are typically used to manage respiratory conditions. While maintaining good respiratory function is important for overall patient care, it's not a primary intervention for an unconscious child with a head injury.
D. Instruct child on performing active range of motion.
Incorrect Explanation: Instructing the child on performing active range of motion is not appropriate for an unconscious child with a head injury.
Explanation: An unconscious child cannot actively perform range of motion exercises. Additionally, it's not a priority intervention in the acute phase of head injury management.
Correct Answer is A
Explanation
Fluid Requirement (mL/24 hours) = Weight (kg) × Fluid Requirement (mL/kg)
Given that the child weighs 70.4 pounds, we first need to convert this weight to kilograms (1 lb = 0.453592 kg):
Weight in kg = 70.4 lb × 0.453592 kg/lb ≈ 31.89 kg
Now, let's calculate the fluid requirement using the given choices:
A) 1740:
Fluid Requirement = 31.89 kg × 55 mL/kg = 1753.95 mL
B) 134056:
This number is significantly larger than any reasonable fluid requirement and is likely an error.
C) 2:
This value is far too low to represent the fluid requirements of a child.
D) 12:
This value is also too low to represent the fluid requirements of a child.
So, the correct answer is A) 1740 mL. The child's estimated daily fluid requirement would be around 1740 mL in a 24-hour period, based on a weight of 70.4 pounds.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today