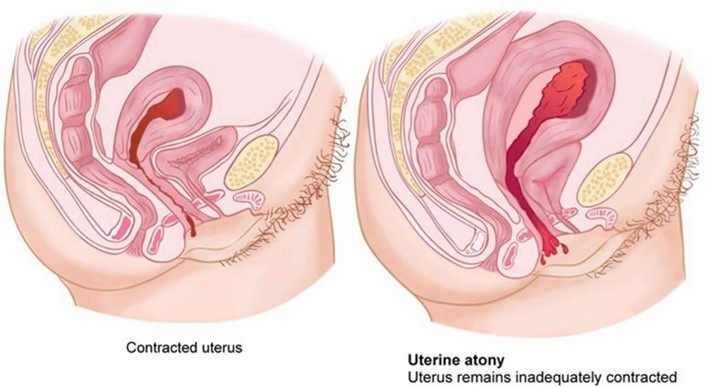
The practical nurse (PN) is caring for a client who delivered 6 hours ago. Assessment findings reveal a boggy uterus that is displaced above and to the right of the umbilicus. Which action should the PN take?
Encourage voiding.
Monitor vital signs.
Notify healthcare provider.
Inspect the perineal pad.
The Correct Answer is A
If the practical nurse (PN) is caring for a client who delivered 6 hours ago and assessment findings reveal a boggy uterus that is displaced above and to the right of the umbilicus, the PN should encourage the client to void. A full bladder can displace the uterus and prevent it from contracting properly, leading to a boggy uterus. Encouraging the client to void can help empty the bladder and allow the uterus to contract and return to its normal position. The other actions listed may also be appropriate in some situations, but encouraging voiding is the most appropriate action in this situation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The action by the PN that is likely to facilitate accurate responses to personal and social history questions is to **request that the mother leave the exam room**. The personal and social history contains many areas of special sensitivity to adolescents including such issues as drug and alcohol use and sexual activity. The teen should provide the personal and social history, not the parent⁴.
Correct Answer is A
Explanation
This can offer a safe place for her and her unborn child. The shelter can also provide resources for counseling and legal assistance if needed.
The safety plan and restraining order are important measures, but the priority should be to ensure the client's immediate safety.
The visit summary documenting the report of abuse is also important, but it should not be the only information provided to the client.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today