Causes of Electrolyte Imbalances
-
Excessive sweating
-
Fluid loss leading to dehydration
-
Excessive vomiting
-
Diuretics like Lasix (K+ depletion)
-
Massive blood loss
-
Dehydration may go unnoticed in hot, dry climates
-
Renal failure
-
It must always be diluted appropriately and never be given IV push.
-
Potassium that is to be given IV should be mixed in the pharmacy and double-checked prior to administration by two nurses.
-
The usual concentration of IV potassium is 2O to 4O mEq/L.
|
Electrolyte |
Derangement |
Causes |
Signs and Symptoms |
Treatment |
Nursing Interventions |
|
Sodium |
Hypernatremia (high sodium) (>145 mEq/L) |
- Diarrhea, vomiting, fever, burns - Diabetes insipidus, kidney disease - High-protein diet, osmotic diuretics - Impaired thirst or mental judgment |
- Excessive thirst - Extreme fatigue, lethargy - Confusion, seizures, coma - Muscle twitching or spasms |
- Treat underlying cause - Replace water deficit with oral or IV fluids - Correct sodium level gradually to avoid cerebral edema |
- Monitor vital signs, fluid status, urine output - Assess neurological and mental status - Provide oral care and hydration - Educate patient on sodium restriction and fluid intake |
|
Sodium |
Hyponatremia (low sodium) (<135 mEq/L) |
- Diuretics, antidepressants, pain medications - Syndrome of inappropriate anti-diuretic hormone (SIADH) - Heart failure, liver cirrhosis, kidney disease - Excessive water intake or retention |
- Headache, nausea, vomiting - Muscle weakness, cramps - Confusion, irritability, restlessness - Seizures, coma |
- Treat underlying cause - Restrict water intake or administer diuretics - Correct sodium level gradually to avoid osmotic demyelination syndrome |
- Monitor vital signs, fluid status, urine output - Assess neurological and mental status - Provide oral care and hydration - Educate patient on fluid restriction and sodium intake |
|
Potassium |
Hyperkalemia (high potassium) (>5 mEq/L) |
- Renal failure, adrenal insufficiency - Acidosis, tissue injury, hemolysis - Potassium-sparing diuretics, ACE inhibitors - Excessive potassium intake or supplements |
- Muscle weakness, paralysis - Nausea, abdominal cramps - Cardiac arrhythmias, cardiac arrest - Paresthesia, anxiety |
- Treat underlying cause - Administer calcium gluconate to stabilize cardiac membrane - Administer insulin and glucose to shift potassium into cells - Administer sodium bicarbonate to correct acidosis |
- Monitor vital signs, cardiac rhythm, ECG changes - Assess muscle strength and reflexes - Monitor potassium level and renal function tests - Educate patient on potassium restriction and medication use |
|
Potassium |
Hypokalemia (low potassium) (<3.5 mEq/L) |
- Diarrhea, vomiting, laxative abuse - Metabolic alkalosis - Diuretics, corticosteroids - Insufficient potassium intake or absorption |
- Muscle weakness, fatigue - Constipation - Cardiac arrhythmias - Paresthesia |
- Treat underlying cause - Replace potassium orally or intravenously - Monitor potassium level and adjust dose accordingly - Correct acid-base imbalance if present |
- Monitor vital signs, cardiac rhythm,< ECG changes - Assess muscle strength and reflexes - Monitor potassium level and renal function tests - Educate patient on potassium-rich foods and medication use |
|
Calcium |
Hypercalcemia (high calcium) (>10.5 mg/dL) |
- Hyperparathyroidism - Malignancy - Vitamin D excess - Thiazide diuretics, lithium, antacids |
- Nausea, vomiting, anorexia - Polyuria, dehydration - Confusion, lethargy, coma - Kidney stones, bone pain |
- Treat underlying cause - Hydrate with saline infusion - Administer loop diuretics to increase calcium excretion - Administer bisphosphonates, calcitonin, or glucocorticoids to lower calcium level |
- Monitor vital signs, fluid status, urine output - Assess neurological and mental status - Monitor calcium level and renal function tests - Educate patient on calcium restriction and hydration |
|
Calcium |
Hypocalcemia (low calcium) (<8.5 mg/dL) |
- Hypoparathyroidism - Vitamin D deficiency - Renal failure - Magnesium deficiency, phosphate excess |
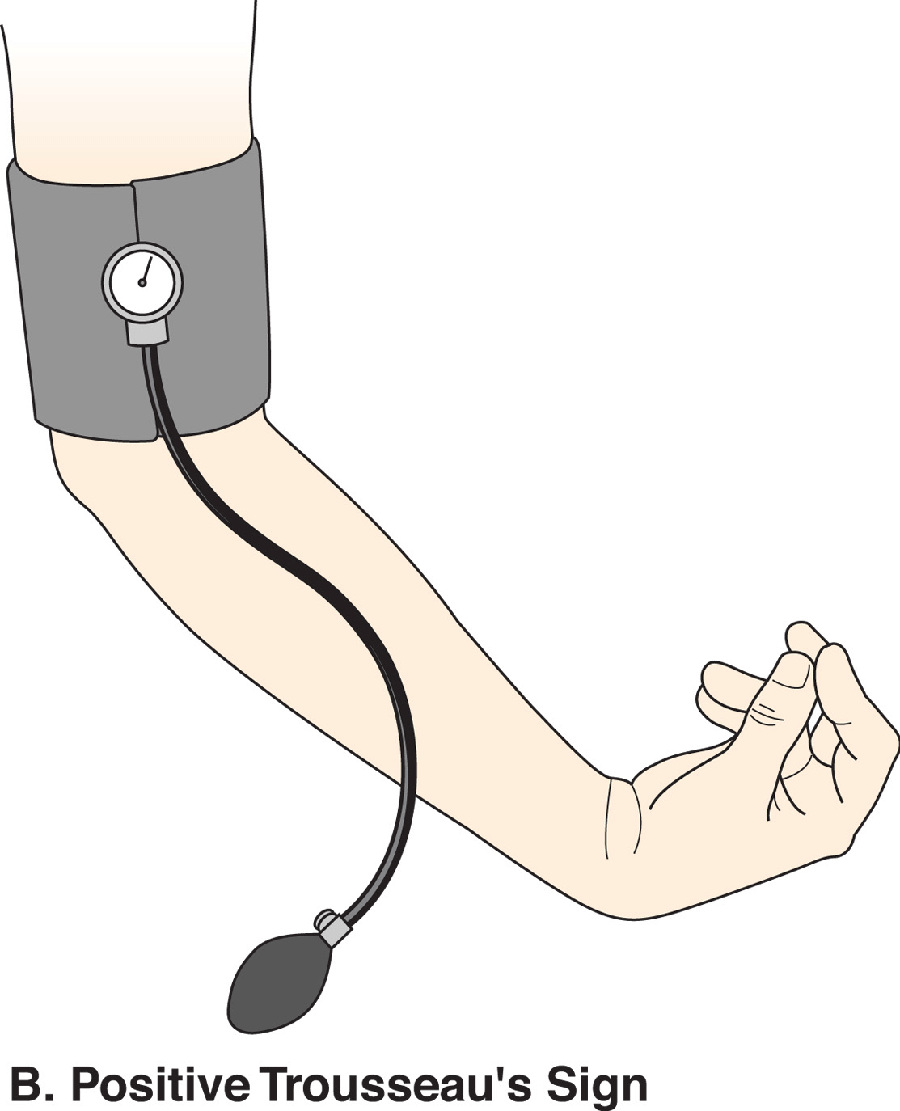
- Muscle cramps, tetany, spasms - Paresthesia, numbness - Cardiac arrhythmias - Positive Chvostek’s or Trousseau’s sign |
- Treat underlying cause - Replace calcium orally or intravenously - Administer vitamin D to enhance absorption - Correct magnesium or phosphate imbalance if present |
- Monitor vital signs, cardiac rhythm,< ECG changes - Assess muscle strength and reflexes - Monitor calcium level and other electrolytes - Educate patient on calcium-rich foods and supplements |
|
Magnesium |
Hypermagnesemia (high magnesium) (>2.5 mEq/L) |
- Renal failure - Adrenal insufficiency - Magnesium-containing antacids or laxatives - Excessive magnesium infusion |
- Hypotension, bradycardia - Muscle weakness, paralysis - Respiratory depression - Lethargy, coma |
- Treat underlying cause - Discontinue magnesium intake or infusion - Administer calcium gluconate to antagonize effects on cardiac muscle - Administer loop diuretics or dialysis to increase magnesium excretion |
- Monitor vital signs, cardiac rhythm,< ECG changes - Assess muscle strength and reflexes - Monitor magnesium level and renal function tests - Educate patient on magnesium restriction and medication use |
Be Alert
Hyperkalemia is usually more dangerous because cardiac arrest is more frequently associated with high serum potassium levels.
Potassium may be given intravenously for severe hypokalemia.
Hypocalcemia
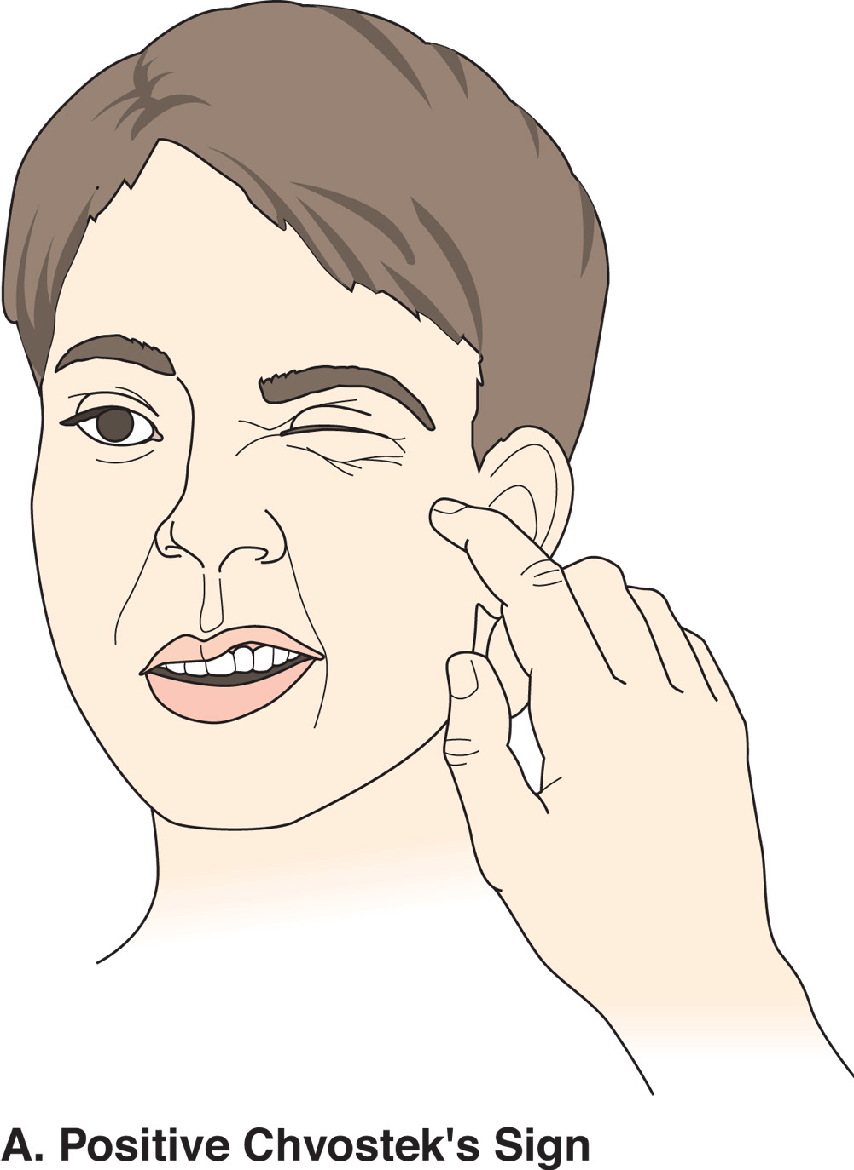
Hypocalcemia
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Questions on Causes of Electrolyte Imbalances