A client receiving parenteral nutrition by central venous access reports feeling unwell. The nurse assesses the client and suspects that the central line has become infected. Which of the following findings indicate that the client has developed a systemic infection? Select all that apply.
Edema
Purulent drainage at intravenous insertion site
Redness at insertion site
Nausea
Leukocytosis
Fever
Correct Answer : B,E,F
Choice A Reason: Edema is not a specific finding of a systemic infection, but rather a possible sign of fluid overload or impaired venous return. It can occur due to excessive infusion rate, heart failure, or obstruction of blood flow in or around the central line.
Choice B Reason: This is a correct choice. Purulent drainage at intravenous insertion site is a finding of a local infection that can spread systemically. It indicates bacterial invasion and inflammation of the skin and subcutaneous tissue around the catheter.
Choice C Reason: Redness at insertion site is a finding of a local infection that can spread systemically. It indicates increased blood flow and inflammation of the skin and subcutaneous tissue around the catheter.
Choice D Reason: Nausea is not a specific finding of a systemic infection, but rather a possible side effect of parenteral nutrition or a symptom of another condition. It can occur due to electrolyte imbalance, hyperglycemia, or gastrointestinal disorders.
Choice E Reason: This is a correct choice. Leukocytosis is a finding of a systemic infection that indicates increased production and release of white blood cells in response to infection. It can be detected by a blood test.
Choice F Reason: This is a correct choice. Fever is a finding of a systemic infection that indicates increased body temperature due to activation of the immune system and release of pyrogens. It can be measured by a thermometer.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
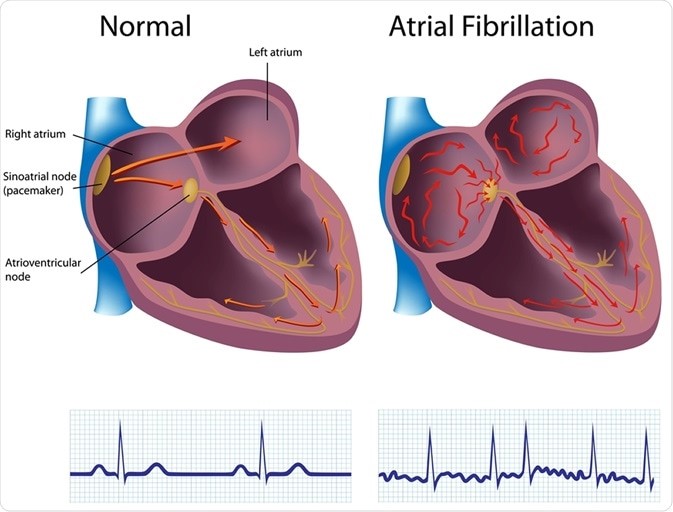
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Correct Answer is A
Explanation
Choice A Reason: "I ate shellfish about 2 weeks ago at a local restaurant." supports the medical diagnosis of hepatitis A, which is an infection of the liver caused by the hepatitis A virus (HAV). HAV is transmitted by fecal-oral route, meaning that it can be contracted by ingesting contaminated food or water, such as raw or undercooked shellfish from polluted waters. The incubation period for hepatitis A is about two to six weeks.
Choice B Reason: "I was an intravenous drug abuser in the past and shared needles." does not support the medical diagnosis of hepatitis A, but may indicate exposure to hepatitis B or C, which are infections of the liver caused by the hepatitis B virus (HBV) or hepatitis C virus (HCV). HBV and HCV are transmitted by blood or body fluids, meaning that they can be contracted by sharing needles, syringes, or other injection equipment with infected people.
Choice C Reason: "I had a blood transfusion in 1980 after major abdominal surgery." does not support the medical diagnosis of hepatitis A, but may indicate exposure to hepatitis B or C, which are infections of the liver caused by the hepatitis B virus (HBV) or hepatitis C virus (HCV). HBV and HCV are transmitted by blood or body fluids, meaning that they can be contracted by receiving blood transfusions or organ transplants from infected donors. However, since 1992, all donated blood in the United States has been screened for HBV and HCV.
Choice D Reason: "I have had unprotected sex with multiple partners." does not support the medical diagnosis of hepatitis A, but may indicate exposure to hepatitis B or C, which are infections of the liver caused by the hepatitis B virus (HBV) or hepatitis C virus (HCV). HBV and HCV are transmitted by blood or body fluids, meaning that they can be contracted by having unprotected sex with infected people. However, sexual transmission of HAV is rare, unless there is contact with fecal matter.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today