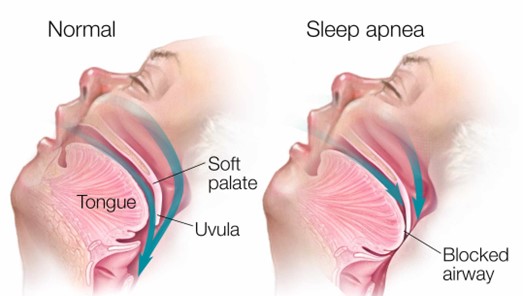
A client with obstructive sleep apnea (OSA) ambulates in the hallway with the nurse prior to bedtime and then returns to bed. Which intervention is most important for the nurse to implement before leaving the client?
Apply the client's positive airway pressure device.
Elevate the head of the bed to a 45 degree angle.
Remove dentures or other oral appliances.
Lift and lock the side rails in place.
The Correct Answer is A
Choice B reason: Elevating the head of the bed to a 45-degree angle is not a sufficient intervention for the nurse to implement before leaving the client. Elevating the head of the bed can help reduce snoring and improve breathing by preventing the tongue and soft palate from falling back and obstructing the airway. However, it may not be enough to prevent apnea episodes in clients with obstructive sleep apnea, especially if they have other risk factors such as obesity, enlarged tonsils, or nasal congestion. The nurse should also use other interventions such as a positive airway pressure device, weight loss, or surgery.
Choice C reason: Removing dentures or other oral appliances is not a relevant intervention for the nurse to implement before leaving the client. Dentures or other oral appliances are devices that replace missing teeth or improve dental alignment. They may help improve speech, chewing, and appearance, but they do not have a direct impact on obstructive sleep apnea. The nurse should instruct the client to remove dentures or other oral appliances before going to bed to prevent discomfort, infection, or damage.
Choice D reason: Lifting and locking the side rails in place is not a necessary intervention for the nurse to implement before leaving the client. Side rails are bars that attach to the sides of the bed frame to prevent falls or injuries. They may provide safety and security for some clients, but they may also pose risks such as entrapment, strangulation, or agitation. The nurse should assess the need for side rails on an individual basis and consider alternative measures such as bed alarms, low beds, or floor mats.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","D","E"]
Explanation
Choice A reason: Providing diet low in phosphorus is not a relevant intervention for a client with cirrhosis of the liver. Phosphorus is a mineral that helps maintain bone health and acid-base balance. Cirrhosis of the liver does not affect phosphorus levels, but it can cause low calcium levels due to impaired vitamin D metabolism. The nurse should provide a diet high in calcium and vitamin D to prevent osteoporosis and fractures.
Choice C reason: Increasing oral fluid intake to 1,500 mL daily is not a suitable intervention for a client with cirrhosis of the liver. Fluid intake should be individualized based on the client's fluid status, electrolyte levels, and urine output. Increasing fluid intake may worsen fluid retention and electrolyte imbalance in clients with cirrhosis of the liver. The nurse should restrict fluid intake to 1,000 to 1,500 mL daily or as prescribed by the healthcare provider.
Correct Answer is C
Explanation
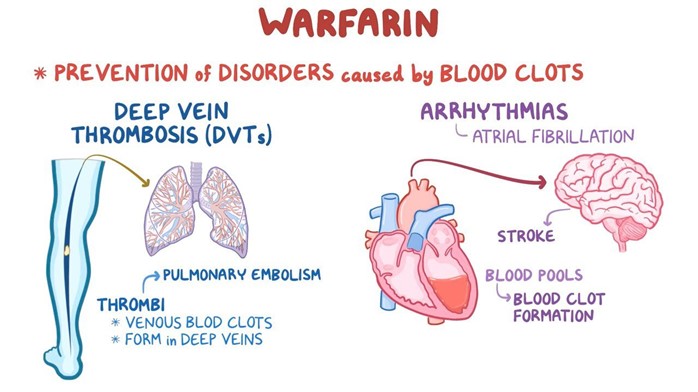
Choice A reason: Increasing the intake of dark green leafy vegetables while taking warfarin is not a good instruction because it can decrease the effectiveness of warfarin. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin.
Choice B reason: Eating two servings of dark green leafy vegetables daily and continuing for 30 days after warfarin therapy is completed is not a good instruction because it can cause bleeding complications. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Stopping warfarin while continuing to eat high amounts of vitamin K can increase the risk of clot formation and thromboembolism.
Choice D reason: Avoiding eating any foods that contain any vitamin K because it is an antagonist of warfarin is not a good instruction because it can cause bleeding complications. Dark green leafy vegetables are rich in vitamin K, which is a coagulation factor that counteracts the anticoagulant effect of warfarin. Eliminating vitamin K from the diet can increase the sensitivity to warfarin and cause excessive bleeding and bruising.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today