A male client who is admitted with bipolar disorder, manic psychosis, is placed in seclusion after unsuccessful attempts to de-escalate him during a sudden mood swing from laughter to jumping and screaming threats while waving a plastic dinner knife.
The client is given haloperidol.
5 mg intramuscularly STAT prior to seclusion.
Which intervention is most important for the nurse to implement immediately after seclusion?
Release the client as soon as composure is regained.
Observe for extrapyramidal symptoms, such as dystonia.
Secure the room with padded walls and minimal furnishings.
Provide one-on-one observation at all times.
The Correct Answer is B
Choice B rationale:
Observing for extrapyramidal symptoms, such as dystonia, is the most important intervention immediately after seclusion because haloperidol is an antipsychotic medication known to have the potential for causing extrapyramidal side effects. Identifying and managing these side effects promptly is crucial to ensure the client's safety.
Choice A rationale:
Releasing the client as soon as composure is regained may not be safe if the client is still at risk of harming themselves or others. Monitoring for the resolution of symptoms and stabilization is important before releasing the client.
Choice C rationale:
Securing the room with padded walls and minimal furnishings is not the immediate priority. While seclusion rooms should be safe and comfortable, observing for potential side effects takes precedence.
Choice D rationale:
Providing one-on-one observation at all times is a resource-intensive intervention and may not be necessary for all clients. Observing for extrapyramidal symptoms is more targeted and appropriate in this scenario.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
A bottle is generally much better than using a pacifier. This statement is not accurate. Prolonged bottle use, especially with sugary liquids like milk, can have adverse effects on a child's dental health. It can lead to an increased risk of cavities, similar to prolonged pacifier use.
Choice B rationale:
The bottle will assist in preventing thumb sucking. This statement is incorrect. While a bottle may provide comfort to a child, it does not prevent thumb sucking. Thumb sucking is a separate behavior that may also have dental implications if it persists beyond a certain age.
Choice C rationale:
Prolonged bottle use can increase the risk for cavities. This response is correct. Prolonged bottle use, especially with milk or sugary beverages, can expose the child's teeth to prolonged contact with sugars, increasing the risk of cavities. It's important for the nurse to educate the mother about the potential dental risks associated with extended bottle use.
Choice D rationale:
Using milk rather than juice helps to avoid tooth decay. While milk is generally considered a healthier choice than juice, the key issue in this scenario is the prolonged use of the bottle, regardless of its content. Prolonged bottle use with any liquid, including milk, can still increase the risk of cavities.
Correct Answer is C
Explanation
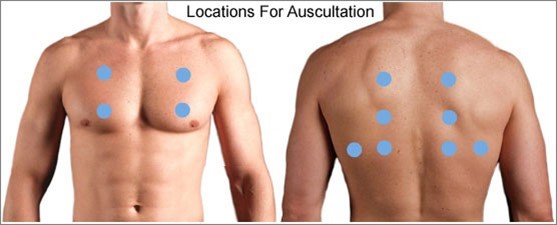
When assessing an older client with left-sided heart failure (HF), the most important intervention for the practical nurse (PN) to implement is to auscultate all lung fields. Left-sided heart failure is characterized by the inability of the left ventricle to effectively pump blood, leading to fluid accumulation in the lungs. Auscultating all lung fields allows the PN to assess for the presence of abnormal lung sounds such as crackles, indicating pulmonary congestion.
Let's evaluate the other options:
a) Inspect for sacral edema.
Sacral edema is commonly associated with right-sided heart failure, not left-sided heart failure. While it is important to assess for edema in clients with heart failure, inspecting for sacral edema may not be the most immediate and crucial intervention in this specific case.
b) Measure urinary output.
Measuring urinary output is a valuable assessment in many clinical situations, but it may not be the most vital intervention in the context of left-sided heart failure. Monitoring urinary output is more relevant in assessing kidney function and fluid balance rather than directly assessing the severity of left-sided heart failure.
d) Check mental acuity.
Checking mental acuity is important in assessing the overall condition of the client, but it is not the most crucial intervention specifically related to left-sided heart failure. Mental status evaluation is more useful in identifying signs of altered mental status or potential complications, rather than directly assessing the impact of left-sided heart failure.
In summary, when assessing an older client with left-sided heart failure, the most important intervention for the practical nurse (PN) to implement is to auscultate all lung fields. This allows for the detection of abnormal lung sounds associated with pulmonary congestion, a hallmark sign of left-sided heart failure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today