A nurse is admitting a client who has active tuberculosis. Which of the following nursing interventions is appropriate?
Place the client in a room that is ventilated to the outside.
Wear a gown when delivering the client's food tray.
Prohibit visitors while the client's infection is active.
Administer a tuberculin skin test prior to discharge.
The Correct Answer is A
A nurse admitting a client who has active tuberculosis should place the client in a room that is ventilated to
the outside. This is an appropriate nursing intervention to prevent the spread of tuberculosis to others.
The other options are not correct.
b) The nurse does not need to wear a gown when delivering the client's food tray but should wear a mask and gloves.
c) Visitors are not prohibited while the client's infection is active but should be limited and should wear masks.
d) A tuberculin skin test is not necessary prior to discharge as the client has already been diagnosed with active tuberculosis.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
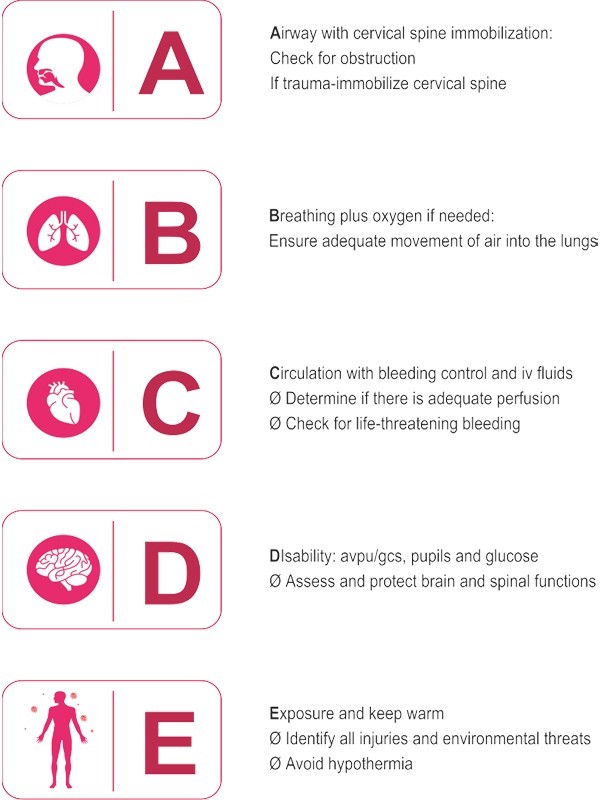
A respiratory rate of 8 breaths per minute with shallow respirations and cyanosis indicates severe respiratory distress or failure. In this situation, the client's oxygenation is compromised, and immediate intervention is needed to ensure an open and unobstructed airway. The nurse should prioritize ensuring the client has a patent airway by assessing for any airway obstruction and taking appropriate measures to clear the airway if necessary. This may involve techniques such as the head tilt-chin lift or jaw thrust maneuver.
While administering oxygen, checking the client's pulse rate, and placing a pulse oximeter on the client's finger are all important interventions in managing respiratory distress, the first and most critical step is to establish a patent airway. Without a clear airway, the client's oxygenation cannot be adequately addressed, and other interventions may be ineffective. Once the airway is secured, the nurse can proceed with providing oxygen, assessing the client's vital signs, and monitoring oxygen saturation using a pulse oximeter.
Correct Answer is C
Explanation
c. Periorbital edema.
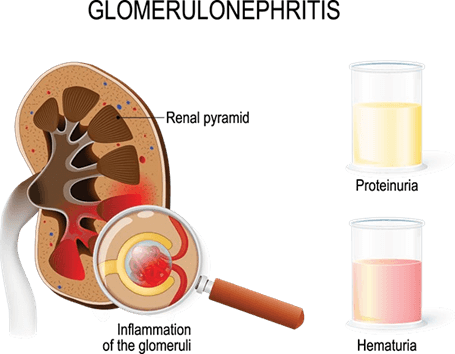
Explanation: Acute glomerulonephritis is an inflammatory condition affecting the glomeruli of the kidneys. It is commonly characterized by periorbital edema, which is swelling around the eyes. This occurs due to fluid retention and impaired kidney function. Other common manifestations of acute glomerulonephritis include hypertension (increased blood pressure), dark or tea-colored urine (hematuria), decreased urine output, and signs of fluid overload such as edema in the hands, feet, and face.
Option a, decreased blood pressure, is not typically seen in acute glomerulonephritis. Instead, hypertension is a common finding due to fluid retention and increased blood volume.
Option b, pale yellow urine, is not expected in acute glomerulonephritis. Instead, urine may appear dark or
tea-colored due to the presence of blood (hematuria).
Option d, increased urination, is not a characteristic finding in acute glomerulonephritis. Instead, there is often a decrease in urine output or oliguria.
It is important to note that individual presentations may vary, and the nurse should consider the complete clinical picture and the child's specific symptoms when assessing for acute glomerulonephritis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today