A nurse is preparing to administer 5 units of regular insulin and 20 units of NPH insulin to a client who has type 1 diabetes mellitus. Which of the following actions should the nurse take first?
Inject 20 units of air into the vial of NPH insulin.
Inject 5 units of air into the vial of regular insulin.
Withdraw 20 units of NPH insulin from the vial.
Withdraw 5 units of regular insulin from the vial.
The Correct Answer is A
Answer: (A) Inject 20 units of air into the vial of NPH insulin.
Rationale:
A) Inject 20 units of air into the vial of NPH insulin:
Injecting air into the vial of NPH insulin is the first step to prevent creating a vacuum, which could make it difficult to withdraw the insulin later. The nurse must inject the corresponding amount of air for the dose needed, ensuring that the insulin can be withdrawn smoothly and accurately without bubbles, which could affect the dose.
B) Inject 5 units of air into the vial of regular insulin:
Injecting air into the regular insulin vial is also necessary before withdrawing the insulin, but it should be done after injecting air into the NPH vial. This sequence ensures that no NPH insulin contaminates the regular insulin vial when the nurse withdraws the doses later.
C) Withdraw 20 units of NPH insulin from the vial:
Withdrawing NPH insulin should be done after air is injected into both vials and after the regular insulin has been drawn up. This sequence prevents the mixing of the two types of insulin and ensures accurate dosing, which is crucial for maintaining the correct blood glucose levels.
D) Withdraw 5 units of regular insulin from the vial:
Withdrawing regular insulin is critical to do before the NPH insulin to prevent contamination of the regular insulin with NPH, which could alter the onset and peak times of the regular insulin. However, it should follow the steps of injecting air into both vials, starting with the NPH vial.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
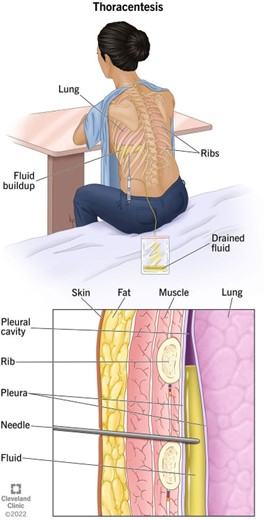
c. "I will have a chest x-ray following the procedure."
Explanation:
The statement that indicates an understanding of the information provided is "I will have a chest x-ray following the procedure."
Explanation for the other options:
a. "I will have general anesthesia during the procedure":
This statement is incorrect. Thoracentesis is typically performed using local anesthesia, which numbs the area where the needle will be inserted. General anesthesia, which induces a state of unconsciousness, is not usually required for this procedure.
b. "I will lie flat for 6 hours following the procedure":
This statement is incorrect. While the client may be advised to lie still for a short period after the thoracentesis, it is not necessary for them to lie flat for a full 6 hours. The specific post-procedure instructions may vary depending on the client's condition and the healthcare provider's preferences.
d. "I will breathe deeply through my nose during the procedure":
This statement is incorrect. During a thoracentesis, the client is typically asked to sit upright and lean forward to allow beter access to the space between the lungs and chest wall. They may be instructed to take slow, deep breaths and hold their breath for short periods as needed during the procedure to help maintain proper positioning and reduce the risk of complications.
In summary, the statement that demonstrates an understanding of the thoracentesis procedure is "I will have a chest x-ray following the procedure." This indicates the client's awareness of the need for a post- procedure chest x-ray to evaluate the results and ensure the absence of any complications.
Correct Answer is C
Explanation
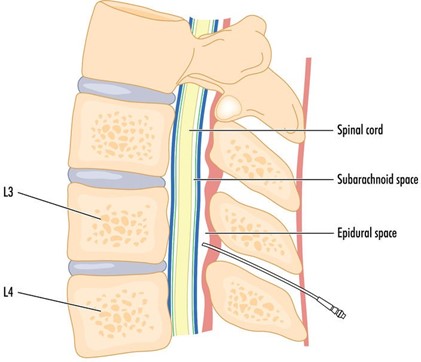
Restlessness is a common sign that a client's pain is not adequately relieved. When a client experience unrelieved pain, they may find it difficult to get comfortable and may exhibit restlessness, such as frequently changing positions, fidgeting, or appearing agitated. It is important for the nurse to assess the client's pain level and address any concerns regarding pain management.
While difficulty swallowing (dysphagia), constipation, and urinary retention can be potential side effects or complications associated with spinal epidural anesthesia, they are not specific indicators of unrelieved pain. These findings may be related to the effects of the anesthesia itself or other factors, and they should still be assessed and addressed by the nurse. However, restlessness is more directly linked to the experience of pain and should be recognized as an important sign that the client's pain relief measures may need adjustment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today