A nurse is assessing a newborn following a vaginal delivery. Which of the following findings should the nurse report to the provider?
Heart rate 136/min
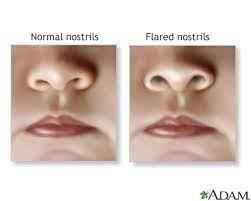
Nasal flaring
Transient strabismus
Overlapping of sutures
The Correct Answer is B
- A. Heart rate 136/min is a normal finding for a newborn. The normal range of heart rate for a newborn is 100 to 160/min.
- B. Nasal flaring is an abnormal finding for a newborn. Nasal flaring indicates respiratory distress and may be caused by conditions such as pneumonia, meconium aspiration, or congenital heart defects.
- C. Transient strabismus is a normal finding for a newborn. Transient strabismus is a temporary misalignment of the eyes that occurs due to weak eye muscles and poor coordination. It usually resolves by 3 to 6 months of age.
- D. Overlapping of sutures is a normal finding for a newborn. Overlapping of sutures is caused by molding of the skull during delivery and allows the head to fit through the birth canal. It usually resolves within a few days after birth.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Respiratory acidosis.
Rationale:
- A. Incorrect. The client does not have respiratory alkalosis because respiratory alkalosis is characterized by a low PaCO2 (less than 35 mm Hg) and a high pH (greater than 7.45).
- B. Incorrect. The client does not have metabolic alkalosis because metabolic alkalosis is characterized by a high HCO3 (greater than 26 mEq/L) and a high pH (greater than 7.45). - C. Correct. The client has respiratory acidosis because respiratory acidosis is characterized by a high PaCO2 (greater than 45 mm Hg) and a low pH (less than 7.35).
- D. Incorrect. The client does not have metabolic acidosis because metabolic acidosis is characterized by a low HCO3 (less than 22 mEq/L) and a low pH (less than 7.35).
Correct Answer is C
Explanation
- A. Incorrect. Organizing the work environment is an important step of the time management process, but it is not the priority. The nurse manager should first identify the activities that need to be done before organizing them.
- B. Incorrect. Delegating assigned tasks appropriately is an important step of the time management process, but it is not the priority. The nurse manager should first determine which tasks can be delegated and which ones require their direct involvement before assigning them to others.
- C. Correct. Making a list of activities to complete is the priority step of the time management process, as it helps the nurse manager to identify and prioritize their goals and responsibilities.
- D. Incorrect. Rewarding yourself for accomplishing goals is an important step of the time management process, but it is not the priority. The nurse manager should first complete the tasks that are essential and urgent before rewarding themselves for their achievements.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today