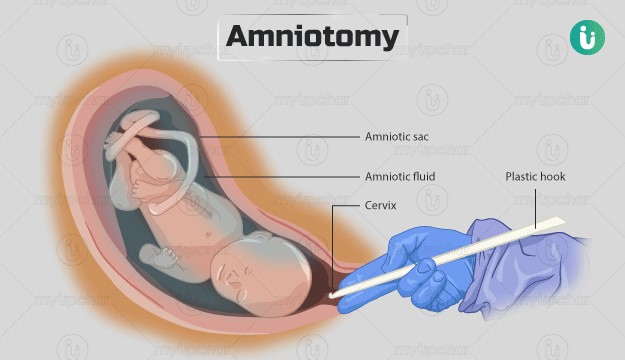
A nurse is assisting in the care of a client following an amniotomy who is now in the active phase of the first stage of labor. Which of the following actions should the nurse take?
Check the client's temperature every 4 hr.
Remind the client to bear down with each contraction.
Maintain the client in the lithotomy position.
Encourage the client to empty the bladder every 2 hr.
The Correct Answer is D
Choice A reason: Check the client's temperature every 4 hr is incorrect, as this action is not frequent enough for a client who had an amniotomy. The nurse should check the client's temperature every 2 hr after an amniotomy, as there is an increased risk of infection due to the rupture of membranes. The nurse should also monitor for signs of chorioamnionitis, such as foul-smelling amniotic fluid, maternal tachycardia, or fetal tachycardia.
Choice B reason: Remind the client to bear down with each contraction is incorrect, as this action is not appropriate for a client who is in the active phase of the first stage of labor. The nurse should instruct the client to avoid bearing down or pushing until they are in the second stage of labor, when the cervix is fully dilated and effaced. Bearing down too early can cause cervical edema, lacerations, or exhaustion.
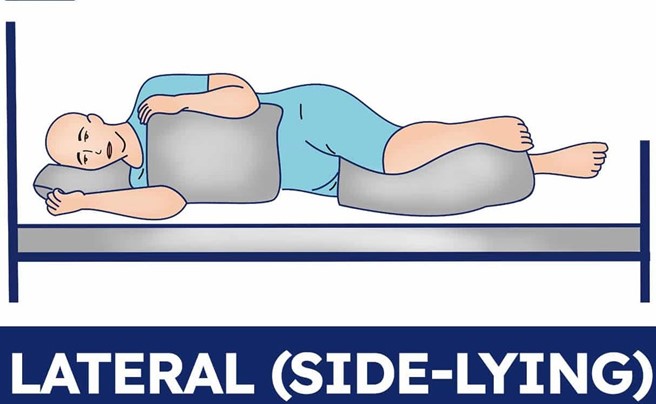
Choice C reason: Maintain the client in the lithotomy position is incorrect, as this action is not optimal for a client who is in the active phase of the first stage of labor. The lithotomy position is a supine position with the legs elevated and abducted, which can reduce blood flow to the uterus and placenta, increase perineal edema, and limit pelvic outlet diameter. The nurse should encourage the client to change positions frequently and use upright or lateral positions that can enhance uterine contractility, fetal descent, and maternal comfort.
Choice D reason: Encourage the client to empty the bladder every 2 hr is correct, as this action can promote labor progress and prevent bladder distension and infection. The nurse should assist the client to void every 2 hr after an amniotomy, as there may be decreased sensation of bladder fullness due to pressure from the fetal head. A full bladder can interfere with uterine contractions, fetal descent, and cervical dilation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason:
Placing the client in a lateral position is the first action the nurse should take, as it can improve maternal and fetal circulation by relieving pressure on the inferior vena cava. The client's blood pressure is low, which can indicate hypotension due to epidural anesthesia or supine hypotension syndrome.
Choice B reason:
Notifying the provider is an important action, as it can facilitate further interventions and monitoring for the client and the fetus. However, this is not the first action the nurse should take, as it does not address the immediate problem of hypotension.
Choice C reason:
Increasing IV fluid rate is an important action, as it can expand blood volume and increase blood pressure. However, this is not the first action the nurse should take, as it may not be effective if the client is in a supine position.
Choice D reason:
Elevating the legs is an important action, as it can enhance venous return and increase blood pressure. However, this is not the first action the nurse should take, as it may worsen supine hypotension syndrome by increasing pressure on the inferior vena cava.
Correct Answer is B
Explanation
Choice A reason: Request the RN perform a cervical examination is incorrect, as this action is not indicated for a client who has a history of genital herpes. A cervical examination can introduce infection and trauma to the cervix and increase the risk of viral shedding and transmission to the fetus. The nurse should avoid performing or requesting a cervical examination unless absolutely necessary.
Choice B reason: Initiate fetal monitoring for baseline and changes is correct, as this action is appropriate for any client who is in labor. Fetal monitoring can provide information about the fetal heart rate, variability, accelerations, decelerations, and contractions. The nurse should monitor the fetal status continuously and report any abnormal findings to the provider.
Choice C reason: Prepare for a vaginal birth is incorrect, as this action may not be possible for a client who has a history of genital herpes. A vaginal birth can expose the fetus to the herpes virus and cause neonatal infection, which can be life-threatening. The nurse should assess the client for signs of active lesions or prodromal symptoms and prepare for a cesarean birth if indicated.
Choice D reason: Administer antibiotics is incorrect, as this action is not effective for a client who has a history of genital herpes. Genital herpes is caused by a virus, not a bacteria, and antibiotics have no effect on viral infections. The nurse should administer antiviral medications as prescribed to reduce viral shedding and transmission to the fetus.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today