A nurse is caring for a client following a cesarean birth. The client tells the nurse that she is hungry. Which of the following actions should the nurse take first?
Offer clear liquids.
Auscultate the client's abdomen.
Check the client's chart for a diet prescription.
Give the client soda crackers.
The Correct Answer is B
Choice B reason:
Auscultating the client's abdomen is the first action the nurse should take, as it can assess the return of bowel function after surgery. The nurse should listen for bowel sounds in all four quadrants, and note their frequency and quality.
Offering clear liquids is an important action, as it can provide hydration and nutrition for the client. However, this is not the first action the nurse should take, as it may cause nausea and vomiting if the client's bowel function has not returned.
Choice C reason:
Checking the client's chart for a diet prescription is an important action, as it can ensure that the client follows the provider's orders and does not consume anything contraindicated. However, this is not the first action the nurse should take, as it does not address the client's hunger or bowel function.
Choice D reason:
Giving the client soda crackers is an important action, as it can provide a bland and easily digestible food for the client. However, this is not the first action the nurse should take, as it may be too solid for the client's stomach if her bowel function has not returned.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
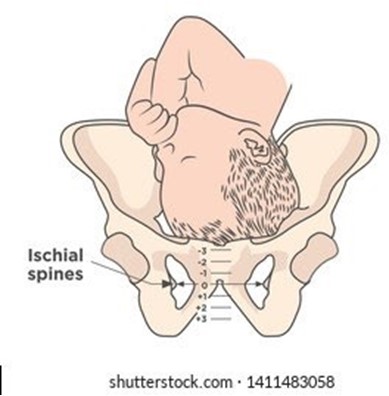
Choice A reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm above the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
Choice B reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm above the ischial spines is correct, as this follows the correct order and measurement of cervical assessment. Cervical dilation, effacement, and station are recorded in that order to describe the progress of labor. Station refers to the relationship between the presenting part of the fetus and the maternal pelvis, measured by the level of the ischial spines. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Choice C reason: The cervix is effaced 3 cm, it is dilated 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not follow the correct order and measurement of cervical assessment. Cervical effacement is measured in percentage, not in centimeters, and it indicates the thinning or shortening of the cervix. Cervical dilation is measured in centimeters, not in percentage, and it indicates the opening or widening of the cervix.
Choice D reason: The cervix is dilated 3 cm, it is effaced 30%, and the presenting part is 1 cm below the ischial spines is incorrect, as this does not match the documentation of station. A negative station means that the presenting part is above the spines, while a positive station means that it is below.
Correct Answer is A
Explanation
Expressions of excitement are typical during the dependent, taking-in phase, which lasts for the first 24 to 48 hr after delivery. The client may relive and review her labor and delivery experience, and may need reassurance and validation from others.
Choice B reason:
Lack of appetite is not an expected finding during the dependent, taking-in phase, as the client may have increased hunger and thirst after delivery. The nurse should encourage adequate nutrition and hydration to promote healing and lactation.
Choice C reason:
Eagerness to learn newborn care skills is more characteristic of the dependent-independent, taking-hold phase, which begins around the third day postpartum. During this phase, the client becomes more confident and interested in caring for herself and her newborn.
ChoiceD reason:
Focus on the family unit and its members is more characteristic of the interdependent, letting-go phase, which occurs after the first week postpartum. During this phase, the client redefines her role within the family and society, and integrates the newborn into her life.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today